





- Filgotinib + Methotrexate Reduces Pain Among Patients With RA and Inadequate Treatment Response
- Increased CV Risk With Short-Term Methylphenidate in Younger Patients With ADHD
- Age and Medication Consumption Impact Headache Disorder Burden
- 2016 CDC Opioid Guideline Led to Unintended Vascular Consequences in Patients With Sickle Cell Disease
- Excessive Internet Use Tied to More Absences for Teens
- Neighborhood Disadvantage Tied to Shorter Breast Cancer-Specific Survival
query object
array(20) {
[0]=>
int(110503)
[1]=>
int(104777)
[2]=>
int(104722)
[3]=>
int(101618)
[4]=>
int(101246)
[5]=>
int(101149)
[6]=>
int(100940)
[7]=>
int(100328)
[8]=>
int(100049)
[9]=>
int(70794)
[10]=>
int(117674)
[11]=>
int(117455)
[12]=>
int(117407)
[13]=>
int(117280)
[14]=>
int(117112)
[15]=>
int(116973)
[16]=>
int(116821)
[17]=>
int(116606)
[18]=>
int(116552)
[19]=>
int(116358)
}
feature query posts
array(4) {
[0]=>
object(WP_Post)#7828 (24) {
["ID"]=>
int(117674)
["post_author"]=>
string(5) "45554"
["post_date"]=>
string(19) "2024-04-26 09:15:00"
["post_date_gmt"]=>
string(19) "2024-04-26 13:15:00"
["post_content"]=>
string(11664) "
In the demanding and emotionally-charged field of health care, physicians often find themselves at the forefront of providing care and support to patients and their loved ones. While empathy and compassion are essential qualities in this profession, the constant exposure to suffering and the pressure to deliver optimal care can take a toll on the emotional well-being of health care professionals. These concerns are particularly true in certain environments like palliative care settings.1 In addition, intense workloads and limited resources during the COVID-19 pandemic further highlighted the mental health crisis facing many health care workers.2
A specific form of psychological distress known as compassion fatigue has emerged as an important topic in need of further research and attention. Compassion fatigue is a state of emotional exhaustion that can reduce your capacity for empathy,1 ultimately putting patient care at risk. To remain effective, health care professionals need strategies to identify the signs of compassion fatigue and alleviate its symptoms before the cumulative stress of work takes over.
How to Recognize Compassion Fatigue
Compassion fatigue is a psychological and physical state that occurs when health care professionals become emotionally drained from their efforts to care for patients. It is often a result of prolonged exposure to patients' suffering, traumatic events, or the inability to alleviate their pain. Experts have defined compassion fatigue as a combination of secondary traumatic stress and burnout.1 It may be viewed as, “the phenomenon of stress resulting from exposure to a traumatized individual rather than from exposure to the trauma itself.”3
As physicians experience increased levels of stress and burnout, they may feel emotionally detached and helpless, losing their sense of purpose. Some warning signs you shouldn't ignore include:
- Apathy and cynicism: A growing sense of pessimism may develop, affecting interactions with patients, colleagues, family, and friends.
- Decreased job satisfaction: Compassion fatigue often leads to frustration and dissatisfaction with one's profession, increasing absenteeism and making physicians question their career choices.3
- Emotional withdrawal: Physicians may emotionally detach themselves from patients and colleagues, leading to numbness or indifference towards their work.
- Physical exhaustion: Feeling constantly tired, irritable, or experiencing sleep disturbances, along with a lack of enthusiasm for work, are signs of compassion fatigue.
- Reduced empathy: A once empathetic physician may find it challenging to connect with patients emotionally, leading to a decline in the quality of care provided.
Studies suggest that the greatest mental health concerns for health care providers during the pandemic included insomnia, anxiety, depression, post-traumatic stress disorder, and stress.2 Untreated compassion fatigue and mental health issues can lead to unhealthy coping strategies, including drug and alcohol use disorders.3
Physicians need to remember that their well-being matters. No one is immune to the weight of such significant responsibility. Getting lost in caring for others isn't sustainable. In fact, doing so may compromise patient care, resulting in widespread negative consequences both personally and professionally.2
Preventing Compassion Fatigue
Physicians can use proactive strategies to combat compassion fatigue that promote self-care and emotional resilience. Physicians must prioritize self-care by taking regular breaks, engaging in hobbies, maintaining a healthy work-life balance, and setting boundaries to protect their well-being. Practicing mindfulness and meditation techniques can help physicians stay present and grounded.4
The opposite of compassion fatigue, referred to as “compassion satisfaction” describes pleasure experienced from relieving patient suffering and enjoying a positive work environment.1 Perhaps one of the best ways to avoid compassion fatigue is by focusing on the satisfying aspect of work, taking time to document and reflect on the positive effects of your efforts, even if they seem small in the larger context of a patient’s eventual outcomes.
Seeking professional counseling or therapy can be immensely beneficial in processing emotional challenges and building coping mechanisms. Counseling can be an opportunity to share small wins and talk through traumatizing experiences. In addition, open communication and sharing with colleagues can create a supportive environment where physicians can seek guidance and understanding. Hospitals and medical institutions should provide training and education on compassion fatigue to help combat this increasing problem for physicians around the world.5
More experienced physicians who take time for their mental wellness can positively impact the culture of medicine by setting a healthier example for students and residents entering the field. As research, awareness, and resources related to compassion fatigue increase, the stigma of mental health care should continue to decrease.5
Alleviating Compassion Fatigue
Despite best efforts, compassion fatigue in health care can seem unavoidable. Physicians must first acknowledge and accept that they are experiencing compassion fatigue. Denying or ignoring these feelings can exacerbate the problem.
It is crucial to lean on support systems, whether it be friends, family, colleagues, or professional counselors. Supervisors can also be a supportive resource. Talking about emotions and seeking understanding can help reduce the burden.1 In addition, therapy can help physicians understand their boundaries and limitations, including the fact that it’s not always possible to change a patient’s outcome or circumstances.1 To shift the focus to compassion satisfaction, physicians must find ways to see the rewards and accomplishments in their work.1
Long shifts and physical exhaustion often make it harder to weather the demands of working in health care. Therefore, time off to rest is vital. Physicians should not hesitate to use their leave entitlements when needed. Time off is critical to staying engaged and should be viewed as a necessary aspect of the job. It should also be used wisely as an active time to rejuvenate. In addition, activities that promote relaxation and joy, such as physical exercise, fun hobbies, or spending time in nature, can help reduce stress levels so you can bring your best self to work.1
Resources for Physician Self-Care
Many health care providers face unrealistic expectations, traumatic experiences, and a challenging work environment. Fortunately, more institutions and organizations recognize and provide resources to address burnout and compassion fatigue. If you're struggling with compassion fatigue (or simply trying to prevent it), you may want to seek out some of the following resources:
- Employee assistance programs (EAPs): Many health care facilities offer EAPs that provide confidential counseling and support services for employees facing emotional challenges.
- Peer support groups: Some medical institutions organize support groups for physicians to share their experiences, struggles, and coping strategies in a safe and understanding environment.
- Therapy: Many medical societies and organizations provide access to professional counseling services specialized in supporting health care professionals.
- Wellness workshops and retreats: Hospitals and medical associations often conduct workshops and seminars on stress management and promoting physician well-being.
Helping Yourself to Help Others
Compassion fatigue is a significant challenge faced by health care professionals, particularly physicians, who dedicate their lives to caring for others. By recognizing the signs of compassion fatigue, taking preventive measures, and utilizing available resources, physicians can safeguard their emotional well-being and continue providing exceptional patient care.
Acknowledging and addressing compassion fatigue is not a sign of weakness but a demonstration of strength and dedication to your profession and patients. Unfortunately, despite an increased awareness of physician burnout and compassion fatigue, there’s still no official guidelines for treatment.5 More research into this common phenomenon can help promote the development of more effective interventions.3 By promoting a culture of understanding, and support, health care institutions can contribute to a healthier and more resilient workforce, improving physicians’ lives and patient outcomes.
" ["post_title"]=> string(61) "Compassion Fatigue: What to Do When Care Becomes Overwhelming" ["post_excerpt"]=> string(129) "Preventing compassion fatigue or managing it when it occurs can be difficult in the high stress environment of the medical field." ["post_status"]=> string(7) "publish" ["comment_status"]=> string(6) "closed" ["ping_status"]=> string(6) "closed" ["post_password"]=> string(0) "" ["post_name"]=> string(49) "compassion-fatigue-when-care-becomes-overwhelming" ["to_ping"]=> string(0) "" ["pinged"]=> string(0) "" ["post_modified"]=> string(19) "2024-04-25 21:34:01" ["post_modified_gmt"]=> string(19) "2024-04-26 01:34:01" ["post_content_filtered"]=> string(0) "" ["post_parent"]=> int(0) ["guid"]=> string(45) "https://www.clinicalpainadvisor.com/?p=117674" ["menu_order"]=> int(0) ["post_type"]=> string(4) "post" ["post_mime_type"]=> string(0) "" ["comment_count"]=> string(1) "0" ["filter"]=> string(3) "raw" } [1]=> object(WP_Post)#7827 (24) { ["ID"]=> int(117455) ["post_author"]=> string(5) "45459" ["post_date"]=> string(19) "2024-04-19 11:05:00" ["post_date_gmt"]=> string(19) "2024-04-19 15:05:00" ["post_content"]=> string(17634) "Exercise has long been considered a core component of conservative treatment for osteoarthritis (OA).1 Health organizations — including the Arthritis Foundation,2,3 Centers for Disease Control and Prevention,4 American College of Sports Medicine (ACSM),5,6 and the Osteoarthritis Action Alliance7 — have strongly encouraged individuals with OA and those at risk of developing OA to stay regularly active, advertising the many benefits of exercise for people with this condition.
How exactly does exercise benefit people with OA? What exactly is happening at the joint and molecular level to achieve these benefits?
Exercise Increases Joint Range of Motion
As mentioned in a previous Rheumatology Advisor article, OA results in neuronally-mediated pain responses that promote natural behaviors, such as aversion to and avoidance of pain-inducing activities and self-imposed immobilization in an attempt to thwart further pain exacerbation. Though counterintuitive, immobilization can further promote joint stiffness and changes in viscosity of the synovial fluid inside the joint.
Normal joint synovial fluid contains high concentrations of hyaluronan,8,9 which plays a key role in cartilage biomechanics. Hyaluronan is a polysaccharide that increases joint lubrication and synovial viscosity into the synovial cavity.8 The presence of sufficient amounts of hyaluronan in the synovial fluid reduces the coefficient of friction between the articular cartilages during motion of the joint.10,11
"
Though counterintuitive, immobilization can further promote joint stiffness and changes in viscosity of the synovial fluid inside the joint.
Results of an animal study conducted by Ingram et al discovered that synoviocytes synthesize and secrete hyaluronan in response to cyclic movement of the joint.8 Joint immobilization reduced the concentration of hyaluronan in the synovial fluid,9 decreasing joint lubrication and synovial viscosity and increasing the coefficient of friction between articular cartilages of the synovial joints. Immobilization also decreased the activity and presence of synovial intimal cells compared with active controls, suggesting the existence of mechanosensitive homeostatic mechanisms.9
Synovial fluid exhibits non-Newtonian flow characteristics, meaning fluid viscosity either increases as the fluid is subjected to a low shear rate over time (rheopectic effect) or the fluid viscosity decreases with exposure to a high shear rate (shear-thinning effect).The viscous dissipation effect refers to heat generation from irreversible work done by fluid motion to overcome layers of shear forces in the flow. This viscous dissipation effect manifests as an increase in synovial fluid temperature.10
A case study conducted by Hor et al demonstrated this viscous dissipation effect occurring in the synovial fluid, following oscillations of an artificial hip joint — a finding quite pertinent to patients with OA who have undergone joint replacements.10 This also explains the concept of injections of shear-thinning, hyaluronan-based fluid hydrogels into the synovium of patients with OA to delay the need for arthroplasty.12
Repetitive oscillating movements that occur during walking or daily joint movement increase the joint temperature as heat is generated, both from muscle contractions and the viscous dissipation effect in the synovial fluid. Movement also stimulates the production of hyaluronan, which lubricates the joint and increases ease of motion with a lowered coefficient of friction at the articular surfaces.
These findings explain one of the cardinal symptoms reported by patients with OA: joint stiffness that is typically worse first thing in the morning or after prolonged periods of inactivity. However, they often report that this stiffness and the accompanying pain improves gradually after repeatedly moving the joint.
Flexibility and stretching exercises also help to restore the length-tension balance of the muscles surrounding joints affected by OA. Individuals with OA are prone to developing contractures. However, routine stretching and flexibility training have been found to improve joint range of motion and functional mobility, as well as reduce OA-related contractures and pain with moderate-quality evidence, according to a systematic review and meta-analysis of the literature conducted by Campbell et al.13
Targeted flexibility exercises may also benefit patients with OA prior to arthroplasty.14 Orthopedic surgeons often refer patients with OA to a physical therapist for preoperative assessment of functional impairments, customized exercise recommendations, and a preoperative physical therapy program for the purpose of optimizing surgical outcomes.
Exercise Improves Muscle Strength and Activation
Exercises that progressively strengthen muscles can have numerous benefits for individuals with OA. Arthrogenic muscle inhibition and motor weakness are neurally-mediated consequence of OA disease processes that cause pain, swelling, and inflammation, which in turn activate nociceptor and mechanoreceptor discharges that prevent full activation and contraction of muscles surrounding the affected joints. This neural inhibition can contribute to muscle weakness and atrophy15 and presents as a significant challenge to effective rehabilitation in patients with OA, even after surgery.16
In one study, Rice et al reported that individuals with OA demonstrated γ-loop dysfunction compared against those without OA.15 This finding may explain the marked quadriceps weakness and atrophy seen with arthrogenic muscle inhibition. Muscles around the joints affected by OA do not demonstrate normal motor unit recruitment secondary to dysfunctional spinal reflex pathways, such as the gamma-loop spindle system,16,17 the flexion reflex,16 and the group I nonreciprocal inhibitory pathway.16 Neuromuscular electrical stimulation, transcutaneous electrical nerve stimulation, and cryotherapy in conjunction with pain-relievers and anti-inflammatory therapies may help patients with OA overcome this barrier to muscle activation.16
Other aspects that may accelerate the progression of OA are joint instability18 and impaired neuromuscular control around the joint, as evidenced by impaired varus-valgus proprioception in individuals with medial knee OA.19 Some patients may be at greater risk of developing OA due to ligamentous laxity and proprioceptive impairment, either from previous joint injuries18 or genetic comorbidities, such as connective tissue disorders.20 Other individuals with OA may demonstrate impaired neuromuscular stabilization of the affected joint.19
Muscle strengthening can restore proprioceptive awareness and increase neuromuscular stabilization of the joint by balancing the strength of the periarticular muscles and offloading stress on the articular cartilage.18 Results of a randomized controlled trial (RCT) by Mikesky et al demonstrated that strength training for 30 months compared with range of motion exercises alone resulted in a decreased mean rate of joint space narrowing, implying that increased muscle strength delayed the progression of OA.21
In terms of exercise frequency, duration, and intensity, 3 or more exercise therapy sessions per week demonstrated increased effectiveness for addressing OA-related symptoms and impairments, compared with sessions occurring less than twice per week; although, exercising twice per week may be more acceptable for individuals who are new to exercise or who have more comorbid conditions.22 The ACSM currently recommends the following exercise prescription for individuals with hip and knee OA: 2 sessions per week with 2 to 4 sets of 8 to 12 repetitions at an intensity between 60% to 80% of the individuals 1-repetition maximum for exercises customized to address muscle strength deficits.22
Therapeutic Exercise and Manual Therapy Provide OA Pain Relief and Improve Functional Mobility
Current evidence suggests that muscle strengthening, flexibility exercises, and manual therapy effectively reduce OA-related pain and disability.23-26 If land-based exercises with full loading of the joint are too painful, water-based exercises may allow individuals with OA to stay physically active, while offloading the painful joint.27
Physical therapists prescribe home exercises so that individuals can independently maintain and progress the gains made during therapy sessions. Continuation of these exercises is critical to prevent loss of function, optimize outcomes, and prevent the return of OA symptoms among this population.27
Proprioception/Balance/Kinesiophobia
In a comparative study, Mani et al found that individuals in the earliest stages of knee OA demonstrated loss of proprioception in the hip and ankle joints.28 Lack of neuromuscular and proprioceptive control over adjacent joints can increase stress at the knee joint, potentially accelerating OA disease progression. Studies have also indicated that OA itself can contribute to reduced proprioceptive capabilities due to dysfunctional articular mechanoreceptors, particularly in severe cases of OA.29
Loss of proprioception, arthrogenic muscle inhibition, and avoidance of painful exercise fuels kinesiophobia — the fear of moving. Individuals with OA report a significant fear of falling and injury related to loss of proprioception and decreased range of motion.30 Kinesiophobia, in turn, accelerates disuse atrophy and muscle weakness by discouraging functional mobility, allowing OA to progress.
Weight Loss Through Exercise May Slow OA Progression
Decreased desire or ability to move due to OA-related pain or symptoms may result in increased sedentary lifestyles and weight gain. Weight gain increases joint compressive forces from external reaction forces due to increased load and the larger muscle contractions that are generated.31
Messier et al reported that knee joint compressive forces increase 4-fold for every pound increase in body weight.32 According to another study by Felson et al, the effect of body weight on the progression of knee OA depends on limb alignment. Moderate degrees of knee joint malalignment (genu valgus or varus) together with excess loading due to increased body weight elevated compartmental pressure in the knee joint. This elevated pressure amplified the risk for structural progression of knee OA, resulting in increased articular cartilage and meniscal degradation in compartments with decreased joint space.33
Disease-Modifying Effects of Exercise on OA
Interestingly, both overuse34,35 and disuse34,36,37 of joints contribute to the physiological degradation of the cartilage by upregulating matrix metalloproteinases in articular cartilage, resulting in tissue degradation.34 Excessive mechanical loading activates the gremlin-1-NF-κB pathway, contributing to OA pathogenesis via cartilage degeneration.35 Similarly, mechanical unloading and immobilization induce thinning of the articular cartilage by accelerating aggrecan catabolism and matrix mineralization in chrondrocytes, as well as cartilage matrix degradation and resorption via subchondral osteoclasts.36 Immobilization also alters proteoglycan synthesis.37
Located in the extracellular matrix of cartilage, proteoglycans retain water, giving cartilage the biomechanical ability to absorb high compressive loads. Proteoglycans also protect and regulate the activity of proinflammatory chemicals, growth factors, and morphogens during remodeling and repair of cartilage following tissue injury. Both OA disease processes and joint immobilization trigger proteoglycan degradation and loss of the extracellular matrix, resulting in severe changes to cartilage homeostasis.38
To combat these degenerative changes seen in OA, moderate loading of the joints promotes and maintains integrity of the articular cartilage.34 Results of an RCT conducted by Roos et al revealed that individuals at risk for knee OA who participated in moderate exercise demonstrated increased proteoglycan content in their knee cartilage, as seen on gadolinium-enhanced magnetic resonance images taken after completing supervised exercise 3 times per week for 4 months.39
Moderate loading of the joints is essential to prevent OA progression. Exercise itself can have disease-modifying effects with less likelihood of harmful side effects or unsustainable outcomes, compared with the long-term pharmacological management of symptoms.40-42
Low Impact Exercises
Both excessive joint loading and immobilization contribute to the progression of OA. Healthcare professionals who specialize in movement rehabilitation and exercise prescription, such as physical therapists, can guide individuals with OA by developing a customized therapeutic exercise program to optimize outcomes. This can simultaneously minimize pain, weight gain, and other negative effects while improving strength, range of motion, balance, and functional mobility.39
It is important to educate individuals with OA about the need to avoid exercises that may cause further harm to the joint integrity, encouraging avoidance of repetitive, high impact activities such as running and jumping.43 Walking, cycling, swimming, and water aerobics are low impact activities that reduce stress on the affected joints while also providing moderate amounts of joint loading, movement, and strengthening.4
In short, motion is lotion for osteoarthritic joints. And exercise really is medicine.
" ["post_title"]=> string(71) "Benefits of Exercise for the Treatment and Management of Osteoarthritis" ["post_excerpt"]=> string(96) "Exercise has long been considered a core component of conservative treatment for osteoarthritis." ["post_status"]=> string(7) "publish" ["comment_status"]=> string(6) "closed" ["ping_status"]=> string(6) "closed" ["post_password"]=> string(0) "" ["post_name"]=> string(41) "benefits-exercise-treatment-management-oa" ["to_ping"]=> string(0) "" ["pinged"]=> string(0) "" ["post_modified"]=> string(19) "2024-04-19 12:32:10" ["post_modified_gmt"]=> string(19) "2024-04-19 16:32:10" ["post_content_filtered"]=> string(0) "" ["post_parent"]=> int(0) ["guid"]=> string(45) "https://www.clinicalpainadvisor.com/?p=117455" ["menu_order"]=> int(0) ["post_type"]=> string(4) "post" ["post_mime_type"]=> string(0) "" ["comment_count"]=> string(1) "0" ["filter"]=> string(3) "raw" } [2]=> object(WP_Post)#7823 (24) { ["ID"]=> int(117407) ["post_author"]=> string(5) "45553" ["post_date"]=> string(19) "2024-04-12 11:15:00" ["post_date_gmt"]=> string(19) "2024-04-12 15:15:00" ["post_content"]=> string(32325) "This physician forum is the second part of a 2-part feature on health care for transgender and gender-divergent youth in the United States. The first part outlines the current legislative climate surrounding pediatric gender-affirming care and the health consequences of anti-trans laws.
The following transcription of our physician forum has been edited for clarity and length.
Matthew Eck: Welcome to today's virtual forum in which we will be discussing gender-affirming hormone therapy for transgender and gender-diverse children. My name is Matthew and I will be your moderator today. Before we dive into our questions, I would like to go around and invite each of our brilliant guests to introduce themselves and share a brief description of their current appointments. Let's start with you, Dr Forcier.
Michelle Forcier, MD, MPH: My name is Michelle Forcier. I use “she” and “they” pronouns. I am a pediatrician, but I've been providing gender, sex, and reproductive health care for over 25 years. I am located on the East Coast, and I am a clinician for Folx Health, and I consult across a lot of different agencies.
ME: Thank you, Dr Forcier. How about you, Dr Bethin?
Kathleen Bethin, MD, PhD: Hi, I am Kathy Bethin. I am a pediatric endocrinologist at University of Buffalo, and I've been a pediatric endocrinologist for, like, 25 years. I do all of endocrine, but I'm the lead for our gender health clinic.
ME: Amazing. Thank you, Dr Bethin. And finally, Dr Shumer.
Daniel Shumer, MD: Hi, I am Dan Shumer, I use “he/him” pronouns. I'm also a pediatric endocrinologist and I work at the University of Michigan as the Clinical Director for the Child and Adolescent Gender Clinic. And I've been involved in gender care since the beginning of my career.
ME: All right, thank you, Dr Shumer. I'm going to go ahead and jump into our first question.
What factors do you consider when initiating a pediatric patient on hormone therapy? Do any patient-specific factors influence your opinion on the risk-benefit ratio of hormone therapy?
MF: I think the way I look at gender care and initiating hormone therapy is [that] gender care is a part of human development, it's a part of primary care. It really is a part of understanding how people grow…their hormones, pre-puberty and puberty, adulthood, into their elder years. It's also a way of understanding where people are in terms of their social, emotional, and cognitive development.
Starting people on gender hormones or gender care is really a matter of where they are in the process of knowing who they are, what their gender identity is, and where they are in their gender identity development. And then [determining] if they require anything that is medical, or if they just require more conversation, support, and resources.
So the sort of primary care approach is, first of all, just finding out who the patient is, listening to their gender narrative, and looking at their support and family and resources. And from there coming up with a strategic plan that is developmentally appropriate.
ME: Thank you for sharing, Dr Forcier. Dr Bethin, would you like to add anything to that?
KB: Yeah, I like to get their story of when this began and try to see where they are and have a discussion. I encourage people to refer even the young kids, just so we can talk and let them know what to expect in the future. And then I ask them to come back once a year, just so we can touch base and see if they're still thinking that way.
And most of the time people come to me and they want hormone therapy, but there are even teenagers that are like, “I'm still thinking about this.” And so we just have a conversation and decide when they're ready.
ME: Thank you, Dr Bethin. How about you, Dr Shumer? Would you like to add anything to that?
DS: Sure. I think the first thing I wanted to say is that having a difference in gender identity, itself, is not a medical problem. It's not a mental health problem. But if someone has a difference in their gender identity, and that difference is causing them distress in their life or impairment in certain social or school activities, making it harder for them to function, contributing to poor mental health — there’s a term for that, and it's called gender dysphoria.
When I'm thinking of gender dysphoria as a medical problem, I'm thinking to myself, that's not too dissimilar to other medical problems, like anxiety, for example. If someone has anxiety, you might say, “Well, what's the goal of treatment?” The goal of treatment would be to reduce the anxiety. “What are the treatment options?” There [are] a lot of non-medical treatment options, like seeing a therapist, or avoiding things that make you anxious, or going for a run. And if those things are helpful, and the anxiety is reduced, then that's terrific. But in the case that it's not, you might also consider a medical intervention, like an anti-anxiety medicine, with the goal of reducing the anxiety and improving well-being. And if you decided to use a medical intervention, then you would re-evaluate that as you used it and re-evaluate that every time you saw the patient for anxiety.
If I'm extrapolating that to gender dysphoria as a medical problem, you say, “Well, there [are] lots of treatment options for gender dysphoria.” There's using a name or pronouns that feel most comfortable for you. There's picking clothes out in the morning that make you feel most confident going out to school. When you pick out your clothes in the morning, you might not be thinking, “I'm treating my gender dysphoria today.” But that's sort of how I think of it. You can talk to a therapist about how to cope with the feelings that you're having related to gender.
And I think it's just really important to say something that I think Dr Forcier touched on, which is that not everyone with a difference in gender identity needs or wants to see a doctor. But it's really when someone is having a difference in gender identity and having challenges with that — because their body is either changing in a way that is not in keeping with their gender identity and that's increasing their distress or making it harder for them to function like other children, or not developing the pubertal changes that other people with that gender are experiencing all around them — that [is when] a medical intervention could be considered.
And just like any other medical decision, just like deciding on an anti-anxiety pill, then you have a conversation with [the patient], including what are their personal factors, their other health concerns, their goals. Talk about the potential benefits of the intervention, talk about the potential risks of the intervention, and then make a decision with them and their family about whether starting that medical intervention could be the right next step for them or not.
ME: Thank you so much, Dr Shumer. That segues nicely into our next question when you brought up gender dysphoria and mental health struggles among transgender and gender-diverse youth.
How do you reconcile the potential clinical challenges of hormone therapy (such as loss of bone mineral density, infertility, and consent) while also considering how trans youth experience disproportionate rates of depression, anxiety, and suicidality?
KB: I talk to them about all of these items. I talk about how important it is for your bone health to get vitamin D and calcium and that any pausing of puberty is not healthy for [your] bones. And I remind them that we can't do this forever. Some patients are non-binary, or gender fluid, and that's great that I can block puberty for them, but at some point you have to allow either male or female hormones because it's not good for your bones.
And I talk about fertility, but that's one thing that is a little problematic because they're all too young to decide for sure that they don't want to have biological children. So, I bring it up every time. I'm like, “Okay, you're still good with adopting if you want children?” And I do talk about [the] research, that there might be new ways to have biological children in the future. But I think it's important to keep bringing it up so that they realize that as long as we continue on this path, there is the possibility that [they] won't have biological children.
ME: Thank you, Dr Bethin. Dr Shumer, do you have anything you would like to add to that?
DS: Yeah, I think there was a lot in your question. You talked about bone health. You talked about fertility… [You talked about] consent. I think that we could spend a whole session talking about all of those topics.
I think that, as Dr Bethin pointed out, you do gain bone density [through] exposure to sex hormones. And that's true, whether it's your endogenous hormones or hormones that are provided during gender transition. If you… measure a 12-year-old’s bone density and it's normal, [then] you take that person and put them on pubertal suppression and you re-measure their bone density at age 13, their [dual energy X-ray absorptiometry] score will be lower because you’re comparing them to other 13-year-olds who are now all going through puberty.
But that person will not be on pubertal suppression forever, and once they come off of their blockers or start hormones, there will be resumption of faster bone density accrual. I think that the takeaway, for me, is not to put someone on blockers for longer than they need to be [and] always thinking about the balance of risks and benefits and having open and candid conversations with them about these things, as Dr Bethin mentioned.
I think fertility is a different conversation, depending on the situation and the age. When you have older adolescents that are presenting to care, there [are] options of fertility preservation prior to starting hormones. When you're using pubertal suppression at the earliest stages of puberty, you're having a conversation about endogenous puberty — that your own puberty is required for fertility to occur, and that endogenous puberty has to happen at some point if you want to achieve fertility.
But these conversations have to be had at an age-appropriate level, and also with the parents. At the end of the day, in the room, the fertility conversation can be more or less meaningful to different patients and families. When we're thinking about what's the risk and what's the benefit, if someone feels that the risk of progressing through an unwanted puberty is, for them, so significant and the fertility question isn't of concern, then they may choose to start on pubertal suppression.
But as was mentioned, this is a conversation that doesn't end at the first visit. It's something that needs to continue over time, and [making sure] that patients and parents are understanding these topics, [in] an age-appropriate way, is an important part of our job as doctors in general, but especially in this area of medicine.
I think that when you mentioned the word consent, in the United States, the definition of consent is someone over 18 choosing a medical path. So when we're thinking of children, we use the word assent. And when we're talking with children and their parents about these topics, the parents are proxies for consent. They're consenting to the care that their child is receiving.
I always think [that] the person in the room that's most knowledgeable about the patient [is] the patient. The person that is second most knowledgeable is the parent or guardian, and I'm a distant third — so I really value the input from parents and conversations with parents about what makes the most sense. But we also need the child's assent, and that means that in an age-appropriate way, they're able to understand the medical decision that we're making, that they agree, and that we are continually re-evaluating that assent and understanding at each visit.
ME: Thank you for that, Dr Shumer. Dr Forcier, do you have anything you would like to add to this conversation?
MF: You all put it so well. I think the 2 things I would add are that it really is about 1) risk and perspective and 2) aspects of timing and what we know. And again, you all have addressed that in terms of risk and perspective — the risk of going through the wrong puberty and all the sequelae that we know happens to folks who are not supported in their gender identity over the years vs the risks of either puberty blockers or other gender-affirming hormones, which are usually pretty… safe and effective methods of either temporarily pausing or blocking puberty or starting an affirmation process.
I think the other piece is [that] there are things that we know and things we don't know. We know that support for youth who are wanting to affirm a diverse gender identity is really important. Whether it's family, whether it's community providers, [support is] an important part of their care. What we don't know is we can't predict anybody's fertility. I can't look at a person and say, “You're fertile, and you're not fertile.” There are things that we can't predict. I can't predict that for this 14-year-old, maybe when they're 26 there'll be an aspect of mourning that they don't have their own uterus and they can't carry their own pregnancy. There are things that we can't necessarily predict or know. And we have to act sometimes in the moment of what is the right next best course for this patient, knowing that as pediatric patients and young adult patients, following them over time and adjusting the course of care is really important.
But it comes down to what Daniel was saying, again, listening to that patient. Kids may be minors, but they also know their own experience. They also understand their own lives. And again, parents know their kids, and having those conversations about what's right for them and balancing those risks and benefits and perspective is just so important. Medicine tends to focus on risks, and when we're talking about gender care in the media, the risks are hyperbolized and overdramatized.
That's why the medicine and this type of care should stay [with] the medical provider. It should stay in the patient room with the patient, the parents, and a clinically trained person.
ME: Thank you, Dr Forcier. This next question is particularly for you, Dr Forcier.
All 3 of you have very considerable academic appointments. How would you describe the changes in the medical education system from when you were in medical school to today, regarding health care for trans youth? Are there any current gaps in the education system? What can students and educators do to close these gaps?
MF: Yes! That's an easy way to answer that question — there are lots of gaps. There's lots of opportunities as a pediatrician. I'm all about looking toward the positive and what can we do vs looking at alternatives, and there's a huge potential for change. Gender care is part of human development and we should all [know] about human development as medical providers, gender care, primary care — all of us carry gender hormones.
So, issues of gender and sexuality being a part of being human and development can be integrated into all aspects of medical training. It doesn't have to be a special unit or 3 talks on gender care. It can be integrated into the cardiology case, and it can be integrated into the prenatal care case. It can be integrated into a whole host of normative medical training experiences as we move through. It is important that there [are] times where gender care is especially attended to because it has not traditionally been included in medical curriculum, and because it is a hot topic, in terms of provision of care and in terms of resources and legislation.
Students love gender care. They are ready to go. Medical students want to learn about gender care, they want to be gender affirmative, they want to be gender savvy. And for me, that's one of the most hopeful things about that question — there is a young generation of patients who understand that gender diversity is a normal part of human development and that we are all uniquely gendered because it is a part of individual identity. And there's a whole new group of providers that are ready to go in terms of working with patients and families to provide this care.
ME: Dr Shumer, Dr Bethin, do either of you have anything to add to what Dr Forcier has already touched upon?
DS: One of the joys of my job is [that] I get to be the course director for a medical student elective called “Transgender Health.” And in that elective, our students get to hang out with me, go to the [operating room], go to adult hormone clinics, [and] have some community experiences. We're only able to offer this to 1 student at a time and it's an elective that gets full right away — almost like you're trying to book your Disney trip during spring break and you need to be the first one that logs into the website.
I think that just goes to show that the learners of today are really interested in making care better for gender-diverse populations. And I think a lot of the new initiatives — with regards to including more and more gender training in medical school — have been driven by the medical students themselves because they see that the training is lacking and they know that they need to know this stuff. But the old people — we didn't learn it, and so we don't know how to teach it. So they're trying to find people, like the 3 of us, to step up and be teachers because they want to do better.
I think that, historically, transgender patients have received poor care in our country, [and] people that are transgender are afraid to present to care because they feel like they may be mistreated, or misgendered. In studies of trans folks, [trans people] mentioned that when they go to the doctor, sometimes it feels like they're teaching the doctor, rather than the other way around, about their gender identity; and patients [that are transgender] are sicker before going to the hospital because they wait longer to go because they're afraid of the interactions with the medical community, which had been poor in the past.
In order to do better, we need to teach that youngest generation. But the good news is they're really eager to learn.
KB: And I would have to say that I am so proud of our medical students because they came to us and asked about a trans elective, and we put together something for them and it's a great experience. The young people that have done this rotation are not necessarily going into gender care, but all kinds of different specialties. But they want to learn more about gender health. They formed a group called “OUTpatient,” and at least once a year they have this big get-together where they educate [people] in the community, and it's really nice to see.
ME: Thank you, Dr Bethin. My next question is actually geared toward you specifically.
Some of your presentation and service activities seem to surround helping physicians better understand patients in the context of their community, or where they are in their lives. What do you feel is an overlooked part of the patient-physician discussion surrounding transgender care?
KB: I want to answer a question that I'm not sure that you asked, but I think providers need to ask their patients what they want to be called and how they want to be identified. I think that that's a big missing part of it.
And I'm also answering another question that I don't think you asked, but one of the things I noted was that there [were] a lot of problems because the medical record reflects somebody's dead name if they haven't legally changed it yet. So, I educated our entire Department of Pediatrics, including the registration people and all of the nursing staff and all of the physicians about how important it is to ask people what their preferred name is, what their pronouns are, and to respect that and to look for that in their record.
ME: Dr Shumer, my next question is for you.
How has the current climate surrounding care of trans and gender-divergent youth in the US impacted you or your institution’s approach to working with this population?
DS: I think that the most important tenet that I always think about is that I need to be practicing evidence-based medicine. In this field, we do have evidence to support the notion that patients [who] are struggling with gender dysphoria do better when provided access to gender-affirming care. There [are] longitudinal studies — following patients from before puberty, through pubertal suppression, through hormones, and following outcomes of quality of life and wellbeing — demonstrating improvement in these things. There [are] comparisons of patients that do and do not have access to the care, demonstrating better outcomes for those who do. Retrospective studies of folks that reflect back on whether or not they had access to this care in the past and how they're doing today [are] influenced by that historical access.
And so, when you ask about the climate, I think I always have to go back to keeping the patients front and center in my mind and figuring out with each and every patient what the best course of action may be. While I'm saying that access to gender-affirming care is helpful, it's also not needed for everyone, as I said in the beginning. So really understanding when to apply the care and work with patients about really understanding what they need.
I think that it is hard when there's a lot of misinformation, that patients living in places that are having access problems, I think, are struggling. But what I'll continue to do is point to the evidence and apply appropriate care to the patients that I'm seeing.
"
Yes, do we have lots to learn? Of course, that's just medicine 101. This is patient-centered, consent-based care. That's what we do. We talk to a patient, we figure out what their goals are, what their needs are, how to minimize harm, how to maximize benefit.
Michelle Forcier, MD, MPH
ME: Thank you Dr Shumer. Dr Bethin, Dr Forcier, do either of you have any comments you'd like to add?
KB: I have seen a lot of families moving here from other states where they can't get their treatment any longer. And it's just very heartwarming to see that families are getting up and changing their entire [lives] to help their child affirm their gender.
MF: I think it's also heartbreaking to see persons that don't know medicine, that don't know the evidence — or are outright making misstatements, untruthful statements, for political or personal gain — creating such an atmosphere of distrust, of hatred, of fear. It's not okay to bully children. And a lot of this environment — if we're going to talk about the environment question — is about preventing kids and families from having access to information, from having access to safe and effective therapeutics, from having access to being acknowledged as being an important person as themselves and part of the community. That's an incredible, I think, harm and assault on a particular group of people in our society and our families and lives. And it's wrong.
And I think it's really so scary for kids and families, even if they're not in a state where there's an access problem, they're hearing about it all over the country and all over the world. And even if they have the privilege of being able to move their family, there are people who cannot move. It's always going to be the most disadvantaged that get caught and have the worst end of the deal. And so I think, as a society, as parents, as civic members, as medical providers, that duty to continue to advocate for children, to continue to advocate for particularly vulnerable group[s] of children and [families] is so important.
And like Daniel said, there is evidence. There's evidence that support and listening and authentic self and affirmation have benefits. When people say there's no research and there's no data — that is untrue. And we need to counter it as strongly as the myths and the misinformation that [are] being promoted. Yes, do we have lots to learn? Of course, that's just medicine 101. This is patient-centered, consent-based care. That's what we do. We talk to a patient, we figure out what their goals are, what their needs are, how to minimize harm, how to maximize benefit. It’s nothing shocking or experimental or new. It's taking care of kids and families. It's taking care of patients. And I think it's been waylaid for other purposes.
ME: Thank you all for sharing your experiences and insights today.
Before we wrap up, do any of you have any final thoughts you'd like to share for the group?
DS: I can just share that it's been a privilege to take care of this patient population throughout my career. I think that being a teenager is hard enough by itself, and when you have a difference in your gender identity, that's really hard. So the patients that I'm seeing, especially in light of some of the things we just talked about, are some of the bravest and most courageous people that I've met. And the joy that I get from seeing a patient that was struggling the first time we met, launching out and becoming a happy, healthy, well-adjusted young adult, making their mark on the world — it makes it a pleasure to go to work every single day.
KB: That was so well said and I 100% agree. They come in and they're struggling and after a conversation, you can already see that they're glad that they came. And yes, thank you for saying it so elegantly.
DS: Thank you.
MF: Daniel, you said it very eloquently. It's about being human. It's about being real, and it's about being yourself. We all do better when we're able to be loved and accepted and safe. And gender diverse patients can come see us in these clinical environments to get the medical care and the services they need. But it's also about our community helping kids feel loved and accepted and safe, so every child has the potential to thrive and grow into a super happy, healthy, and wonderful young person and adult.
Disclosures: Michelle Forcier, MD, MPH reported affiliations as a consultant with Folx Health, Planned Parenthood League of Massachusetts, ConferMED, New York University Student Health, and Transhealth. No other speakers declared any potential conflicts of interest.
" ["post_title"]=> string(71) "Physician Forum: Pediatricians Discuss Gender-Affirming Hormone Therapy" ["post_excerpt"]=> string(123) "Three pediatricians shared their experiences providing gender-affirming care to transgender and gender-divergent children. " ["post_status"]=> string(7) "publish" ["comment_status"]=> string(6) "closed" ["ping_status"]=> string(6) "closed" ["post_password"]=> string(0) "" ["post_name"]=> string(15) "physician-forum" ["to_ping"]=> string(0) "" ["pinged"]=> string(0) "" ["post_modified"]=> string(19) "2024-04-12 12:25:34" ["post_modified_gmt"]=> string(19) "2024-04-12 16:25:34" ["post_content_filtered"]=> string(0) "" ["post_parent"]=> int(0) ["guid"]=> string(45) "https://www.clinicalpainadvisor.com/?p=117407" ["menu_order"]=> int(0) ["post_type"]=> string(4) "post" ["post_mime_type"]=> string(0) "" ["comment_count"]=> string(1) "0" ["filter"]=> string(3) "raw" } [3]=> object(WP_Post)#7816 (24) { ["ID"]=> int(117280) ["post_author"]=> string(5) "45562" ["post_date"]=> string(19) "2024-04-05 11:25:00" ["post_date_gmt"]=> string(19) "2024-04-05 15:25:00" ["post_content"]=> string(15525) "Pelvic floor dysfunction (PFD) can negatively impact women with this disorder. The musculature of the pelvic floor is vital for everyday functions. When these muscles no longer work properly, significant distress can occur because of bothersome symptoms such as urinary incontinence, fecal incontinence, pelvic organ prolapse (POP), and sexual dysfunction.
The pelvic floor muscles include the coccygeus, iliococcygeus, pubococcygeus, and puborectalis and form a dome-shaped basin in the pelvis that supports the bladder, colon, uterus, vagina, rectum, and anus (Figure 1).1 In addition to supporting the pelvic organs, these muscles control fecal and urinary continence and play a role in childbirth and sexual function.2 Issues arise when the pelvic floor muscles either contract too much (hypertonicity) or do not contract enough and become lax (hypotonicity).
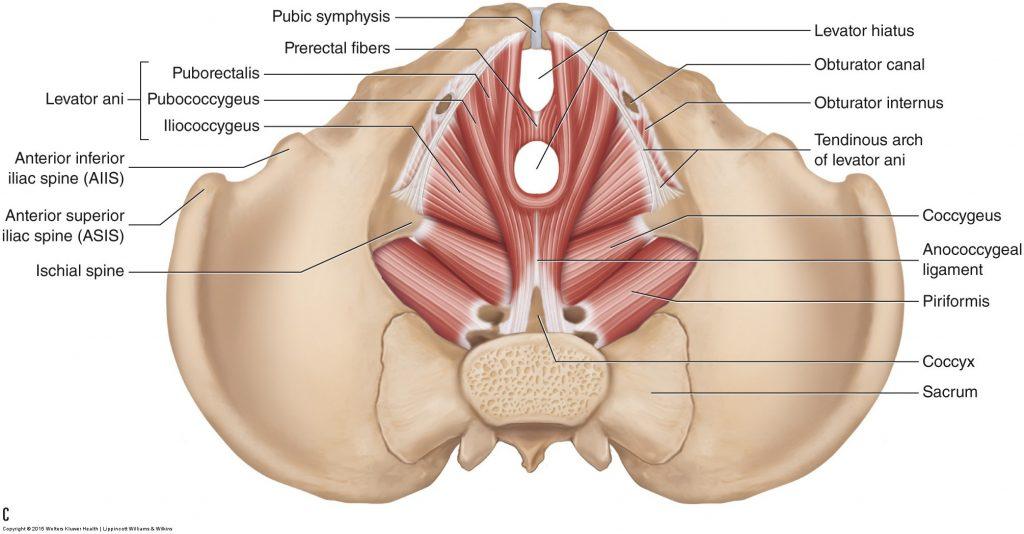
Source: Muscolino J. Learn Muscles. 2017.
© Joe Muscolino. Used with permission from Dr Joe Muscolino.1
There are multiple risk factors for PFD. Trauma to the pelvic region, whether from pregnancy, childbirth, injury, or surgery, can result in damage to the muscles and nerves in the pelvic region. Damage to the nerves that innervate the pelvic floor muscles (S3 and S4) can impair the coordination of the musculature. Additionally, overuse of the pelvic muscles, such as using the restroom too often or straining during excretion, can cause muscle fatigue and lead to PFD. Lastly, obesity raises susceptibility to PFD because it increases intra-abdominal pressure and places excess weight on the pelvic muscles, potentially causing damage over time.2 Because of the numerous risk factors and their prevalence, many women are affected by this condition; in fact, 1 in 4 women will experience PFD in their lifetime.3
The pelvic floor musculature plays a crucial role in many activities of daily living (ADLs) and can cause tremendous distress in the event of dysfunction. The distress of PFD negatively impacts quality of life, namely in 4 areas: physical, psychological, social, and financial.
Effect on Quality of Life
Physical
The physical impact of PFD arises from the bothersome symptoms that occur with the condition. Symptoms differ based on the type of dysfunction the patient is experiencing. If the pelvic floor muscles are hypotonic the patient can experience urinary incontinence or prolapse of the pelvic organs. The symptoms of hypertonic pelvic floor muscles are more variable. These symptoms include difficulty urinating, constipation, and pain with physical or sexual activity.3 These manifestations of PFD are disruptive and impact the physical wellbeing of the person who is experiencing them.
Psychological
Studies have shown an association between PFD and psychological distress, including depression and anxiety.4,5 One study investigated the rates of depression among 100 women diagnosed with PFD compared with 100 women without PFD. The results found that rates of depression among women with PFD were triple that of the women in the control group.4 A study published in 2020 further support the findings of a significant association between PFD and mental health impacts. After reviewing the data from thousands of participants, it was concluded that those with urinary incontinence had higher levels of depression and anxiety compared with the control group.5 The mental health toll of PFD disrupts quality of life by impacting psychological wellness.
Social
Women with PFD can suffer from sexual dysfunction at a greater rate than the general population, and this negatively impacts romantic relationships. In women with PFD, the prevalence of sexual dysfunction is as high as 83%.6 Factors related to PFD that led to higher reports of sexual dysfunction included painful intercourse, negative body image because of pelvic organ prolapse, and fear of incontinence during sexual activity.6 A study invited women with PFD to self-report their sexual function status and severity of their PFD symptoms. The higher a woman ranked her PFD symptoms, the more sexual dysfunction she experienced.7
Financial
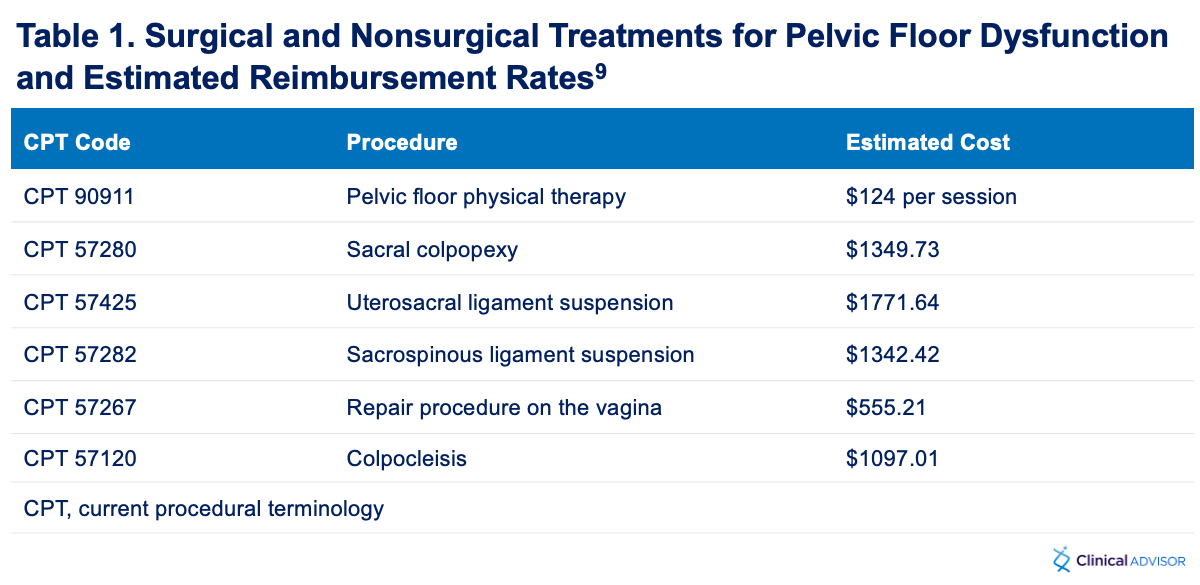
Symptoms of PFD can be disruptive to employment in many ways, such as an increased need for bathroom breaks, episodes of incontinence while at work, needing time off to seek out treatment, etc. Additionally, treatment of the disorder can be expensive. For example, pelvic floor physical therapy is typically used as the first line treatment for PFD. The National Institute of Excellence in Health and Social Services (in the UK) recommends at least 10 pelvic floor physical therapy sessions to address PFD symptoms.8 These sessions can cost hundreds of dollars each. Another treatment option is a pessary. These devices typically range from $50 to $100 in cost and require an in-office visit for proper fitting. The most expensive treatment option is surgical intervention. There are multiple surgical options for PFD (Table 1), but they can be costly. According to the Centers for Medicare and Medicaid Services, the prices of these procedures can range from $500 - $1800.9 These treatments, while successful at managing PFD symptoms, can be financially burdensome for many individuals, especially those without health insurance.
Diagnosis
Early diagnosis leads to prompt treatment, which can help alleviate the burden of PFD symptoms. When a patient presents with pelvic floor symptoms, a thorough medical history can provide clues to the correct diagnosis. It is important to inquire about pelvic trauma, surgical history, childbirth (mode of delivery, number of births, etc), and the nature of the symptoms. The answers to these questions can clue the provider to possible etiologies for PFD.
Following the medical history, a physical should be performed, specifically inspection and palpation. Inspecting the pelvic area while the patient undergoes attempted contraction and relaxation of the pelvic muscles can reveal asymmetries, prolapse, or inability to control the actions of the muscles. Palpation of these muscles may elicit involuntary contraction (spasms), identify areas of weakness, or elicit pain. The aforementioned symptoms/signs are positive findings for PFD.
"
When the muscles of the pelvic floor no longer function properly, it can lead to urinary incontinence, fecal incontinence, sexual dysfunction, and pelvic organ prolapse.
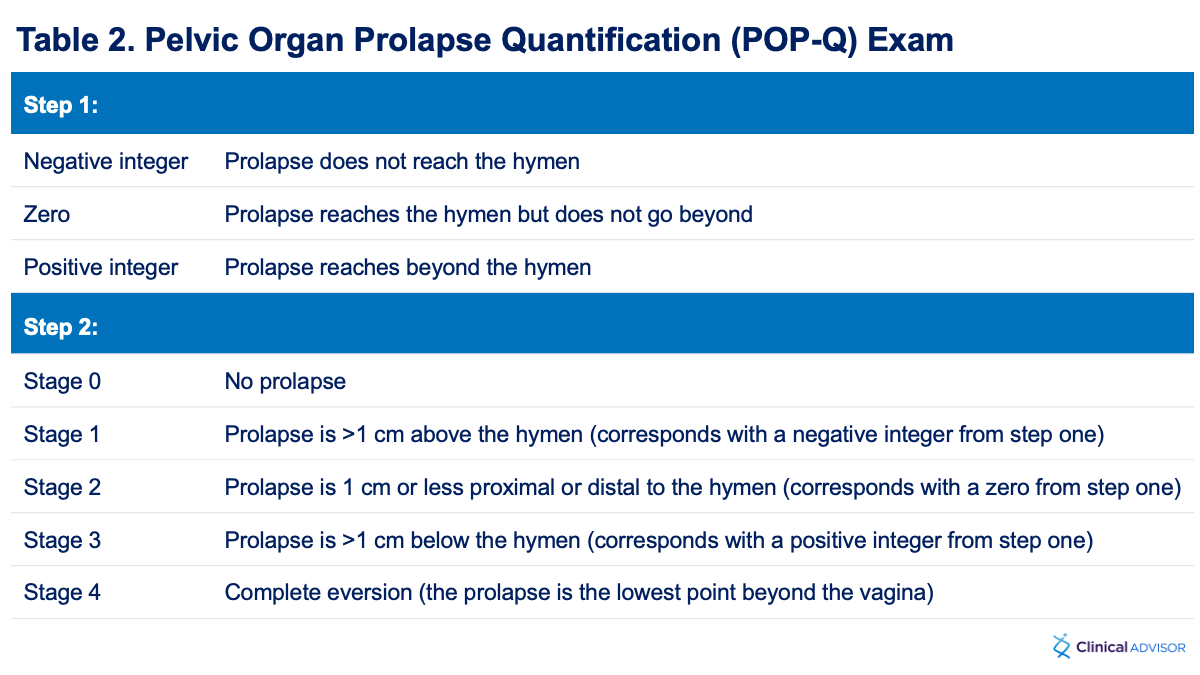
If the primary symptom is prolapse, the pelvic organ prolapse quantification exam (POP-Q) should be referenced to determine the stage and severity of the prolapse (Table 2). The POP-Q exam is divided into 2 parts. During the first part of this exam, the prolapse is measured during Valsalva maneuver and then assigned an integer based on how far the prolapse reaches in relation to the hymen. The second part of the exam includes staging the prolapse based on established criteria. Utilization of the POP-Q exam can help guide treatment.10
Treatment Options
There are multiple options available for the treatment of PFD. Choosing an option should be individualized to address the patient’s primary symptom. It is crucial to customize treatment to maximize the patient’s ability to adhere to treatment, as some treatments may be uncomfortable or costly. Each option should be discussed between the provider and the patient to ensure appropriate care.
Pelvic Floor Physical Therapy
Pelvic floor physical therapy (PT) is the first-line recommendation for treatment and prevention of PFD, either as monotherapy or as adjunctive therapy.11 Physical therapy is highly effective when completed with proper technique and follow-up. The PT regimen should be guided by the patient’s presenting symptoms and aim to improve control of the pelvic floor muscles to ameliorate the symptoms of PFD.12
Weight Loss
Because obesity can play a role in the etiology of PFD, decreasing BMI reduces the risk for developing PFD and the severity of symptoms. Both surgical and nonsurgical weight loss options have been shown to improve the symptoms of PFD.13 Nonsurgical options include diet changes and exercise regimens, both of which should be discussed with the patient.
Pessary
The pessary is inserted into the vagina and provides support to the prolapsed area(s).13 Pessaries come in variable shapes, but the ring pessary and the Gellhorn pessary (Figure 2) are the most widely used for PFD.14 Both types of pessaries decrease symptoms of urinary incontinence and improve prolapse.15 Pessaries require a fitting and require ongoing care to avoid vaginal irritation and infection. With proper education and follow-up, pessaries are suitable treatment options for some forms of PFD.
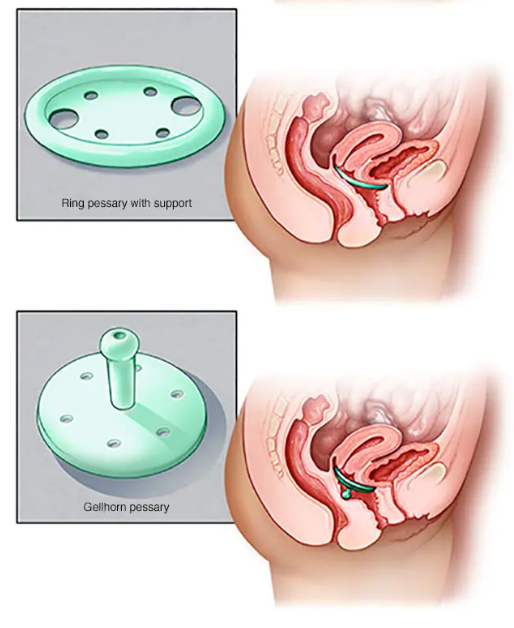
Source: Used with permission of Mayo Foundation for Medical Education and Research. All rights reserved.14
Surgery
Surgery is an option for women with pelvic organ prolapse who are refractory to other treatments, or for those who desire a more immediate response to treatment. There are a multitude of surgical options for these patients and choosing the best option will depend on the type and severity of the prolapse. Some options include sacral colpopexy, uterosacral or sacrospinous ligament suspension, anterior vaginal prolapse repair, posterior vaginal prolapse repair, and colpocleisis.15 Pelvic organ prolapse suspension can greatly improve sexual function in patients with PFD and can improve incontinence.16 One study found that 81% of women with severe prolapse who opted for surgical correction saw significant improvement in their symptoms, and these findings were consistent regardless of the procedure used.17 Surgical options are more invasive and should be discussed on an individual basis to determine what is right for the patient.
Conclusion
The musculature of the pelvic floor is vital for everyday functions. When these muscles no longer work properly, urinary incontinence, fecal incontinence, pelvic organ prolapse, and sexual dysfunction can occur. The result can decrease quality of life by affecting physical, psychological, social, and financial wellbeing. It is important for health care providers to promptly diagnose PFD and tailor treatment to limit the burden the disorder can place on patients.
" ["post_title"]=> string(65) "Female Pelvic Floor Dysfunction and its Effect on Quality of Life" ["post_excerpt"]=> string(147) "The pelvic floor musculature plays a crucial role in many activities of daily living and can cause tremendous distress in the event of dysfunction." ["post_status"]=> string(7) "publish" ["comment_status"]=> string(6) "closed" ["ping_status"]=> string(6) "closed" ["post_password"]=> string(0) "" ["post_name"]=> string(40) "pelvic-floor-dysfunction-quality-of-life" ["to_ping"]=> string(0) "" ["pinged"]=> string(0) "" ["post_modified"]=> string(19) "2024-04-05 12:31:59" ["post_modified_gmt"]=> string(19) "2024-04-05 16:31:59" ["post_content_filtered"]=> string(0) "" ["post_parent"]=> int(0) ["guid"]=> string(45) "https://www.clinicalpainadvisor.com/?p=117280" ["menu_order"]=> int(0) ["post_type"]=> string(4) "post" ["post_mime_type"]=> string(0) "" ["comment_count"]=> string(1) "0" ["filter"]=> string(3) "raw" } }Features
More features
Clinical Tools
Powered by

Powered by 




Intervention Improves HRQOL in Patients With Cancer

Lebanese Oncology Nurses Explore What It Means to Provide Spiritual Care to Patients

CGM Use Linked to Lower Diabetic Retinopathy Risk in Type 1 Diabetes

Use of Radiation Nursing Clinic Increased With Concurrent Chemoradiation for Gynecologic Cancer

About 4 in 10 Adults Choose Telemedicine Visits











