This physician forum is the second part of a 2-part feature on health care for transgender and gender-divergent youth in the United States. The first part outlines the current legislative climate surrounding pediatric gender-affirming care and the health consequences of anti-trans laws.
The following transcription of our physician forum has been edited for clarity and length.
Matthew Eck: Welcome to today's virtual forum in which we will be discussing gender-affirming hormone therapy for transgender and gender-diverse children. My name is Matthew and I will be your moderator today. Before we dive into our questions, I would like to go around and invite each of our brilliant guests to introduce themselves and share a brief description of their current appointments. Let's start with you, Dr Forcier.
Michelle Forcier, MD, MPH: My name is Michelle Forcier. I use “she” and “they” pronouns. I am a pediatrician, but I've been providing gender, sex, and reproductive health care for over 25 years. I am located on the East Coast, and I am a clinician for Folx Health, and I consult across a lot of different agencies.
ME: Thank you, Dr Forcier. How about you, Dr Bethin?
Kathleen Bethin, MD, PhD: Hi, I am Kathy Bethin. I am a pediatric endocrinologist at University of Buffalo, and I've been a pediatric endocrinologist for, like, 25 years. I do all of endocrine, but I'm the lead for our gender health clinic.
ME: Amazing. Thank you, Dr Bethin. And finally, Dr Shumer.
Daniel Shumer, MD: Hi, I am Dan Shumer, I use “he/him” pronouns. I'm also a pediatric endocrinologist and I work at the University of Michigan as the Clinical Director for the Child and Adolescent Gender Clinic. And I've been involved in gender care since the beginning of my career.
ME: All right, thank you, Dr Shumer. I'm going to go ahead and jump into our first question.
What factors do you consider when initiating a pediatric patient on hormone therapy? Do any patient-specific factors influence your opinion on the risk-benefit ratio of hormone therapy?
MF: I think the way I look at gender care and initiating hormone therapy is [that] gender care is a part of human development, it's a part of primary care. It really is a part of understanding how people grow…their hormones, pre-puberty and puberty, adulthood, into their elder years. It's also a way of understanding where people are in terms of their social, emotional, and cognitive development.
Starting people on gender hormones or gender care is really a matter of where they are in the process of knowing who they are, what their gender identity is, and where they are in their gender identity development. And then [determining] if they require anything that is medical, or if they just require more conversation, support, and resources.
So the sort of primary care approach is, first of all, just finding out who the patient is, listening to their gender narrative, and looking at their support and family and resources. And from there coming up with a strategic plan that is developmentally appropriate.
ME: Thank you for sharing, Dr Forcier. Dr Bethin, would you like to add anything to that?
KB: Yeah, I like to get their story of when this began and try to see where they are and have a discussion. I encourage people to refer even the young kids, just so we can talk and let them know what to expect in the future. And then I ask them to come back once a year, just so we can touch base and see if they're still thinking that way.
And most of the time people come to me and they want hormone therapy, but there are even teenagers that are like, “I'm still thinking about this.” And so we just have a conversation and decide when they're ready.
ME: Thank you, Dr Bethin. How about you, Dr Shumer? Would you like to add anything to that?
DS: Sure. I think the first thing I wanted to say is that having a difference in gender identity, itself, is not a medical problem. It's not a mental health problem. But if someone has a difference in their gender identity, and that difference is causing them distress in their life or impairment in certain social or school activities, making it harder for them to function, contributing to poor mental health — there’s a term for that, and it's called gender dysphoria.
When I'm thinking of gender dysphoria as a medical problem, I'm thinking to myself, that's not too dissimilar to other medical problems, like anxiety, for example. If someone has anxiety, you might say, “Well, what's the goal of treatment?” The goal of treatment would be to reduce the anxiety. “What are the treatment options?” There [are] a lot of non-medical treatment options, like seeing a therapist, or avoiding things that make you anxious, or going for a run. And if those things are helpful, and the anxiety is reduced, then that's terrific. But in the case that it's not, you might also consider a medical intervention, like an anti-anxiety medicine, with the goal of reducing the anxiety and improving well-being. And if you decided to use a medical intervention, then you would re-evaluate that as you used it and re-evaluate that every time you saw the patient for anxiety.
If I'm extrapolating that to gender dysphoria as a medical problem, you say, “Well, there [are] lots of treatment options for gender dysphoria.” There's using a name or pronouns that feel most comfortable for you. There's picking clothes out in the morning that make you feel most confident going out to school. When you pick out your clothes in the morning, you might not be thinking, “I'm treating my gender dysphoria today.” But that's sort of how I think of it. You can talk to a therapist about how to cope with the feelings that you're having related to gender.
And I think it's just really important to say something that I think Dr Forcier touched on, which is that not everyone with a difference in gender identity needs or wants to see a doctor. But it's really when someone is having a difference in gender identity and having challenges with that — because their body is either changing in a way that is not in keeping with their gender identity and that's increasing their distress or making it harder for them to function like other children, or not developing the pubertal changes that other people with that gender are experiencing all around them — that [is when] a medical intervention could be considered.
And just like any other medical decision, just like deciding on an anti-anxiety pill, then you have a conversation with [the patient], including what are their personal factors, their other health concerns, their goals. Talk about the potential benefits of the intervention, talk about the potential risks of the intervention, and then make a decision with them and their family about whether starting that medical intervention could be the right next step for them or not.
ME: Thank you so much, Dr Shumer. That segues nicely into our next question when you brought up gender dysphoria and mental health struggles among transgender and gender-diverse youth.
How do you reconcile the potential clinical challenges of hormone therapy (such as loss of bone mineral density, infertility, and consent) while also considering how trans youth experience disproportionate rates of depression, anxiety, and suicidality?
KB: I talk to them about all of these items. I talk about how important it is for your bone health to get vitamin D and calcium and that any pausing of puberty is not healthy for [your] bones. And I remind them that we can't do this forever. Some patients are non-binary, or gender fluid, and that's great that I can block puberty for them, but at some point you have to allow either male or female hormones because it's not good for your bones.
And I talk about fertility, but that's one thing that is a little problematic because they're all too young to decide for sure that they don't want to have biological children. So, I bring it up every time. I'm like, “Okay, you're still good with adopting if you want children?” And I do talk about [the] research, that there might be new ways to have biological children in the future. But I think it's important to keep bringing it up so that they realize that as long as we continue on this path, there is the possibility that [they] won't have biological children.
ME: Thank you, Dr Bethin. Dr Shumer, do you have anything you would like to add to that?
DS: Yeah, I think there was a lot in your question. You talked about bone health. You talked about fertility… [You talked about] consent. I think that we could spend a whole session talking about all of those topics.
I think that, as Dr Bethin pointed out, you do gain bone density [through] exposure to sex hormones. And that's true, whether it's your endogenous hormones or hormones that are provided during gender transition. If you… measure a 12-year-old’s bone density and it's normal, [then] you take that person and put them on pubertal suppression and you re-measure their bone density at age 13, their [dual energy X-ray absorptiometry] score will be lower because you’re comparing them to other 13-year-olds who are now all going through puberty.
But that person will not be on pubertal suppression forever, and once they come off of their blockers or start hormones, there will be resumption of faster bone density accrual. I think that the takeaway, for me, is not to put someone on blockers for longer than they need to be [and] always thinking about the balance of risks and benefits and having open and candid conversations with them about these things, as Dr Bethin mentioned.
I think fertility is a different conversation, depending on the situation and the age. When you have older adolescents that are presenting to care, there [are] options of fertility preservation prior to starting hormones. When you're using pubertal suppression at the earliest stages of puberty, you're having a conversation about endogenous puberty — that your own puberty is required for fertility to occur, and that endogenous puberty has to happen at some point if you want to achieve fertility.
But these conversations have to be had at an age-appropriate level, and also with the parents. At the end of the day, in the room, the fertility conversation can be more or less meaningful to different patients and families. When we're thinking about what's the risk and what's the benefit, if someone feels that the risk of progressing through an unwanted puberty is, for them, so significant and the fertility question isn't of concern, then they may choose to start on pubertal suppression.
But as was mentioned, this is a conversation that doesn't end at the first visit. It's something that needs to continue over time, and [making sure] that patients and parents are understanding these topics, [in] an age-appropriate way, is an important part of our job as doctors in general, but especially in this area of medicine.
I think that when you mentioned the word consent, in the United States, the definition of consent is someone over 18 choosing a medical path. So when we're thinking of children, we use the word assent. And when we're talking with children and their parents about these topics, the parents are proxies for consent. They're consenting to the care that their child is receiving.
I always think [that] the person in the room that's most knowledgeable about the patient [is] the patient. The person that is second most knowledgeable is the parent or guardian, and I'm a distant third — so I really value the input from parents and conversations with parents about what makes the most sense. But we also need the child's assent, and that means that in an age-appropriate way, they're able to understand the medical decision that we're making, that they agree, and that we are continually re-evaluating that assent and understanding at each visit.
ME: Thank you for that, Dr Shumer. Dr Forcier, do you have anything you would like to add to this conversation?
MF: You all put it so well. I think the 2 things I would add are that it really is about 1) risk and perspective and 2) aspects of timing and what we know. And again, you all have addressed that in terms of risk and perspective — the risk of going through the wrong puberty and all the sequelae that we know happens to folks who are not supported in their gender identity over the years vs the risks of either puberty blockers or other gender-affirming hormones, which are usually pretty… safe and effective methods of either temporarily pausing or blocking puberty or starting an affirmation process.
I think the other piece is [that] there are things that we know and things we don't know. We know that support for youth who are wanting to affirm a diverse gender identity is really important. Whether it's family, whether it's community providers, [support is] an important part of their care. What we don't know is we can't predict anybody's fertility. I can't look at a person and say, “You're fertile, and you're not fertile.” There are things that we can't predict. I can't predict that for this 14-year-old, maybe when they're 26 there'll be an aspect of mourning that they don't have their own uterus and they can't carry their own pregnancy. There are things that we can't necessarily predict or know. And we have to act sometimes in the moment of what is the right next best course for this patient, knowing that as pediatric patients and young adult patients, following them over time and adjusting the course of care is really important.
But it comes down to what Daniel was saying, again, listening to that patient. Kids may be minors, but they also know their own experience. They also understand their own lives. And again, parents know their kids, and having those conversations about what's right for them and balancing those risks and benefits and perspective is just so important. Medicine tends to focus on risks, and when we're talking about gender care in the media, the risks are hyperbolized and overdramatized.
That's why the medicine and this type of care should stay [with] the medical provider. It should stay in the patient room with the patient, the parents, and a clinically trained person.
ME: Thank you, Dr Forcier. This next question is particularly for you, Dr Forcier.
All 3 of you have very considerable academic appointments. How would you describe the changes in the medical education system from when you were in medical school to today, regarding health care for trans youth? Are there any current gaps in the education system? What can students and educators do to close these gaps?
MF: Yes! That's an easy way to answer that question — there are lots of gaps. There's lots of opportunities as a pediatrician. I'm all about looking toward the positive and what can we do vs looking at alternatives, and there's a huge potential for change. Gender care is part of human development and we should all [know] about human development as medical providers, gender care, primary care — all of us carry gender hormones.
So, issues of gender and sexuality being a part of being human and development can be integrated into all aspects of medical training. It doesn't have to be a special unit or 3 talks on gender care. It can be integrated into the cardiology case, and it can be integrated into the prenatal care case. It can be integrated into a whole host of normative medical training experiences as we move through. It is important that there [are] times where gender care is especially attended to because it has not traditionally been included in medical curriculum, and because it is a hot topic, in terms of provision of care and in terms of resources and legislation.
Students love gender care. They are ready to go. Medical students want to learn about gender care, they want to be gender affirmative, they want to be gender savvy. And for me, that's one of the most hopeful things about that question — there is a young generation of patients who understand that gender diversity is a normal part of human development and that we are all uniquely gendered because it is a part of individual identity. And there's a whole new group of providers that are ready to go in terms of working with patients and families to provide this care.
ME: Dr Shumer, Dr Bethin, do either of you have anything to add to what Dr Forcier has already touched upon?
DS: One of the joys of my job is [that] I get to be the course director for a medical student elective called “Transgender Health.” And in that elective, our students get to hang out with me, go to the [operating room], go to adult hormone clinics, [and] have some community experiences. We're only able to offer this to 1 student at a time and it's an elective that gets full right away — almost like you're trying to book your Disney trip during spring break and you need to be the first one that logs into the website.
I think that just goes to show that the learners of today are really interested in making care better for gender-diverse populations. And I think a lot of the new initiatives — with regards to including more and more gender training in medical school — have been driven by the medical students themselves because they see that the training is lacking and they know that they need to know this stuff. But the old people — we didn't learn it, and so we don't know how to teach it. So they're trying to find people, like the 3 of us, to step up and be teachers because they want to do better.
I think that, historically, transgender patients have received poor care in our country, [and] people that are transgender are afraid to present to care because they feel like they may be mistreated, or misgendered. In studies of trans folks, [trans people] mentioned that when they go to the doctor, sometimes it feels like they're teaching the doctor, rather than the other way around, about their gender identity; and patients [that are transgender] are sicker before going to the hospital because they wait longer to go because they're afraid of the interactions with the medical community, which had been poor in the past.
In order to do better, we need to teach that youngest generation. But the good news is they're really eager to learn.
KB: And I would have to say that I am so proud of our medical students because they came to us and asked about a trans elective, and we put together something for them and it's a great experience. The young people that have done this rotation are not necessarily going into gender care, but all kinds of different specialties. But they want to learn more about gender health. They formed a group called “OUTpatient,” and at least once a year they have this big get-together where they educate [people] in the community, and it's really nice to see.
ME: Thank you, Dr Bethin. My next question is actually geared toward you specifically.
Some of your presentation and service activities seem to surround helping physicians better understand patients in the context of their community, or where they are in their lives. What do you feel is an overlooked part of the patient-physician discussion surrounding transgender care?
KB: I want to answer a question that I'm not sure that you asked, but I think providers need to ask their patients what they want to be called and how they want to be identified. I think that that's a big missing part of it.
And I'm also answering another question that I don't think you asked, but one of the things I noted was that there [were] a lot of problems because the medical record reflects somebody's dead name if they haven't legally changed it yet. So, I educated our entire Department of Pediatrics, including the registration people and all of the nursing staff and all of the physicians about how important it is to ask people what their preferred name is, what their pronouns are, and to respect that and to look for that in their record.
ME: Dr Shumer, my next question is for you.
How has the current climate surrounding care of trans and gender-divergent youth in the US impacted you or your institution’s approach to working with this population?
DS: I think that the most important tenet that I always think about is that I need to be practicing evidence-based medicine. In this field, we do have evidence to support the notion that patients [who] are struggling with gender dysphoria do better when provided access to gender-affirming care. There [are] longitudinal studies — following patients from before puberty, through pubertal suppression, through hormones, and following outcomes of quality of life and wellbeing — demonstrating improvement in these things. There [are] comparisons of patients that do and do not have access to the care, demonstrating better outcomes for those who do. Retrospective studies of folks that reflect back on whether or not they had access to this care in the past and how they're doing today [are] influenced by that historical access.
And so, when you ask about the climate, I think I always have to go back to keeping the patients front and center in my mind and figuring out with each and every patient what the best course of action may be. While I'm saying that access to gender-affirming care is helpful, it's also not needed for everyone, as I said in the beginning. So really understanding when to apply the care and work with patients about really understanding what they need.
I think that it is hard when there's a lot of misinformation, that patients living in places that are having access problems, I think, are struggling. But what I'll continue to do is point to the evidence and apply appropriate care to the patients that I'm seeing.
"
Yes, do we have lots to learn? Of course, that's just medicine 101. This is patient-centered, consent-based care. That's what we do. We talk to a patient, we figure out what their goals are, what their needs are, how to minimize harm, how to maximize benefit.
Michelle Forcier, MD, MPH
ME: Thank you Dr Shumer. Dr Bethin, Dr Forcier, do either of you have any comments you'd like to add?
KB: I have seen a lot of families moving here from other states where they can't get their treatment any longer. And it's just very heartwarming to see that families are getting up and changing their entire [lives] to help their child affirm their gender.
MF: I think it's also heartbreaking to see persons that don't know medicine, that don't know the evidence — or are outright making misstatements, untruthful statements, for political or personal gain — creating such an atmosphere of distrust, of hatred, of fear. It's not okay to bully children. And a lot of this environment — if we're going to talk about the environment question — is about preventing kids and families from having access to information, from having access to safe and effective therapeutics, from having access to being acknowledged as being an important person as themselves and part of the community. That's an incredible, I think, harm and assault on a particular group of people in our society and our families and lives. And it's wrong.
And I think it's really so scary for kids and families, even if they're not in a state where there's an access problem, they're hearing about it all over the country and all over the world. And even if they have the privilege of being able to move their family, there are people who cannot move. It's always going to be the most disadvantaged that get caught and have the worst end of the deal. And so I think, as a society, as parents, as civic members, as medical providers, that duty to continue to advocate for children, to continue to advocate for particularly vulnerable group[s] of children and [families] is so important.
And like Daniel said, there is evidence. There's evidence that support and listening and authentic self and affirmation have benefits. When people say there's no research and there's no data — that is untrue. And we need to counter it as strongly as the myths and the misinformation that [are] being promoted. Yes, do we have lots to learn? Of course, that's just medicine 101. This is patient-centered, consent-based care. That's what we do. We talk to a patient, we figure out what their goals are, what their needs are, how to minimize harm, how to maximize benefit. It’s nothing shocking or experimental or new. It's taking care of kids and families. It's taking care of patients. And I think it's been waylaid for other purposes.
ME: Thank you all for sharing your experiences and insights today.
Before we wrap up, do any of you have any final thoughts you'd like to share for the group?
DS: I can just share that it's been a privilege to take care of this patient population throughout my career. I think that being a teenager is hard enough by itself, and when you have a difference in your gender identity, that's really hard. So the patients that I'm seeing, especially in light of some of the things we just talked about, are some of the bravest and most courageous people that I've met. And the joy that I get from seeing a patient that was struggling the first time we met, launching out and becoming a happy, healthy, well-adjusted young adult, making their mark on the world — it makes it a pleasure to go to work every single day.
KB: That was so well said and I 100% agree. They come in and they're struggling and after a conversation, you can already see that they're glad that they came. And yes, thank you for saying it so elegantly.
DS: Thank you.
MF: Daniel, you said it very eloquently. It's about being human. It's about being real, and it's about being yourself. We all do better when we're able to be loved and accepted and safe. And gender diverse patients can come see us in these clinical environments to get the medical care and the services they need. But it's also about our community helping kids feel loved and accepted and safe, so every child has the potential to thrive and grow into a super happy, healthy, and wonderful young person and adult.
Disclosures:Michelle Forcier, MD, MPH reported affiliations as a consultant with Folx Health, Planned Parenthood League of Massachusetts, ConferMED, New York University Student Health, and Transhealth.No other speakers declared any potential conflicts of interest.
Pelvic floor dysfunction (PFD) can negatively impact women with this disorder. The musculature of the pelvic floor is vital for everyday functions. When these muscles no longer work properly, significant distress can occur because of bothersome symptoms such as urinary incontinence, fecal incontinence, pelvic organ prolapse (POP), and sexual dysfunction.
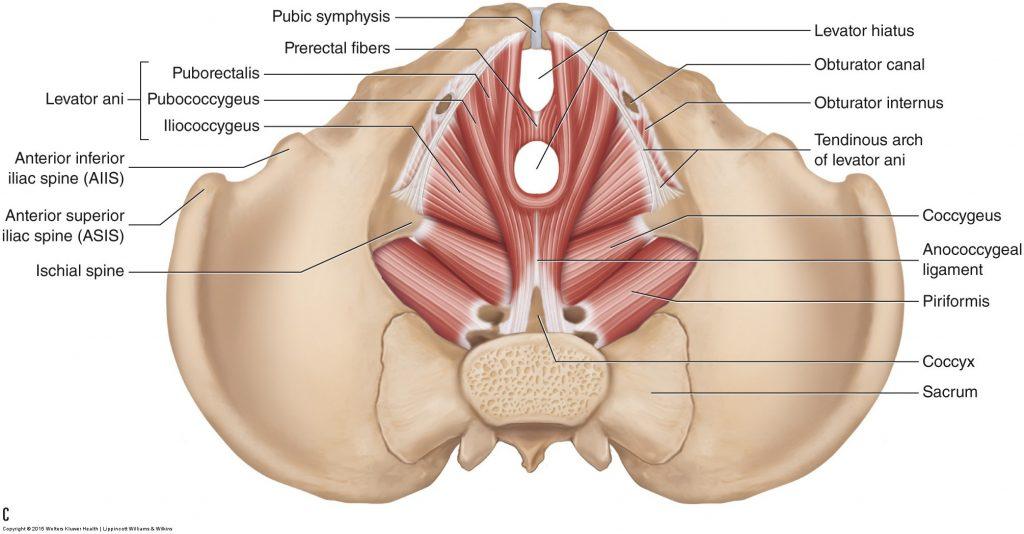
The pelvic floor muscles include the coccygeus, iliococcygeus, pubococcygeus, and puborectalis and form a dome-shaped basin in the pelvis that supports the bladder, colon, uterus, vagina, rectum, and anus (Figure 1).1 In addition to supporting the pelvic organs, these muscles control fecal and urinary continence and play a role in childbirth and sexual function.2 Issues arise when the pelvic floor muscles either contract too much (hypertonicity) or do not contract enough and become lax (hypotonicity).
There are multiple risk factors for PFD. Trauma to the pelvic region, whether from pregnancy, childbirth, injury, or surgery, can result in damage to the muscles and nerves in the pelvic region. Damage to the nerves that innervate the pelvic floor muscles (S3 and S4) can impair the coordination of the musculature. Additionally, overuse of the pelvic muscles, such as using the restroom too often or straining during excretion, can cause muscle fatigue and lead to PFD. Lastly, obesity raises susceptibility to PFD because it increases intra-abdominal pressure and places excess weight on the pelvic muscles, potentially causing damage over time.2 Because of the numerous risk factors and their prevalence, many women are affected by this condition; in fact, 1 in 4 women will experience PFD in their lifetime.3
The pelvic floor musculature plays a crucial role in many activities of daily living (ADLs) and can cause tremendous distress in the event of dysfunction. The distress of PFD negatively impacts quality of life, namely in 4 areas: physical, psychological, social, and financial.
Effect on Quality of Life
Physical
The physical impact of PFD arises from the bothersome symptoms that occur with the condition. Symptoms differ based on the type of dysfunction the patient is experiencing. If the pelvic floor muscles are hypotonic the patient can experience urinary incontinence or prolapse of the pelvic organs. The symptoms of hypertonic pelvic floor muscles are more variable. These symptoms include difficulty urinating, constipation, and pain with physical or sexual activity.3 These manifestations of PFD are disruptive and impact the physical wellbeing of the person who is experiencing them.
Psychological
Studies have shown an association between PFD and psychological distress, including depression and anxiety.4,5 One study investigated the rates of depression among 100 women diagnosed with PFD compared with 100 women without PFD. The results found that rates of depression among women with PFD were triple that of the women in the control group.4 A study published in 2020 further support the findings of a significant association between PFD and mental health impacts. After reviewing the data from thousands of participants, it was concluded that those with urinary incontinence had higher levels of depression and anxiety compared with the control group.5 The mental health toll of PFD disrupts quality of life by impacting psychological wellness.
Social
Women with PFD can suffer from sexual dysfunction at a greater rate than the general population, and this negatively impacts romantic relationships. In women with PFD, the prevalence of sexual dysfunction is as high as 83%.6 Factors related to PFD that led to higher reports of sexual dysfunction included painful intercourse, negative body image because of pelvic organ prolapse, and fear of incontinence during sexual activity.6 A study invited women with PFD to self-report their sexual function status and severity of their PFD symptoms. The higher a woman ranked her PFD symptoms, the more sexual dysfunction she experienced.7
Financial
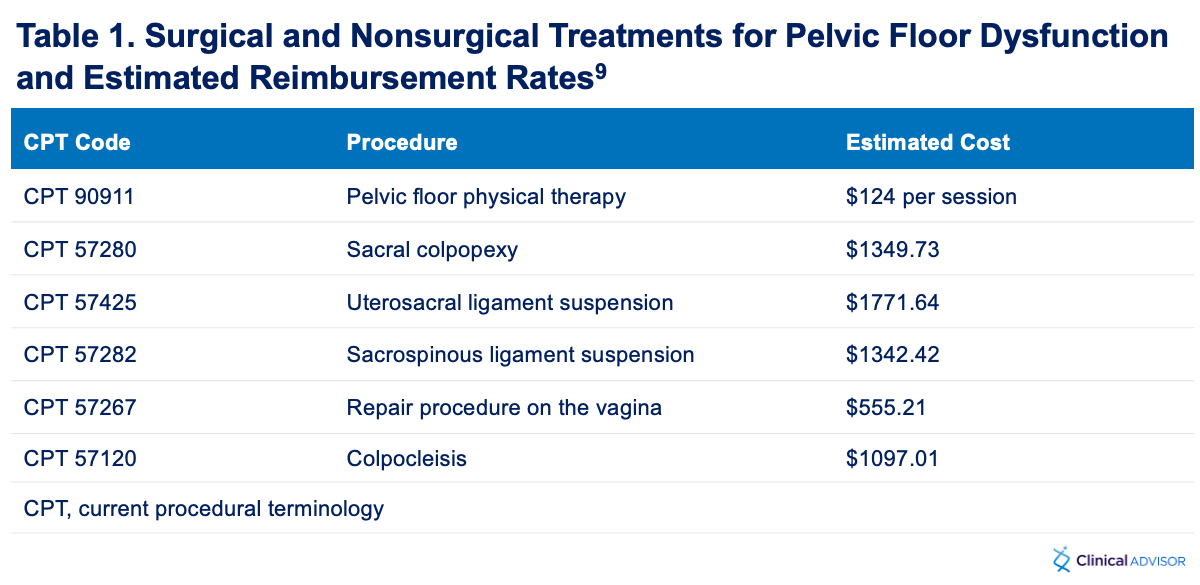
Symptoms of PFD can be disruptive to employment in many ways, such as an increased need for bathroom breaks, episodes of incontinence while at work, needing time off to seek out treatment, etc. Additionally, treatment of the disorder can be expensive. For example, pelvic floor physical therapy is typically used as the first line treatment for PFD. The National Institute of Excellence in Health and Social Services (in the UK) recommends at least 10 pelvic floor physical therapy sessions to address PFD symptoms.8 These sessions can cost hundreds of dollars each. Another treatment option is a pessary. These devices typically range from $50 to $100 in cost and require an in-office visit for proper fitting. The most expensive treatment option is surgical intervention. There are multiple surgical options for PFD (Table 1), but they can be costly. According to the Centers for Medicare and Medicaid Services, the prices of these procedures can range from $500 - $1800.9 These treatments, while successful at managing PFD symptoms, can be financially burdensome for many individuals, especially those without health insurance.
Diagnosis
Early diagnosis leads to prompt treatment, which can help alleviate the burden of PFD symptoms. When a patient presents with pelvic floor symptoms, a thorough medical history can provide clues to the correct diagnosis. It is important to inquire about pelvic trauma, surgical history, childbirth (mode of delivery, number of births, etc), and the nature of the symptoms. The answers to these questions can clue the provider to possible etiologies for PFD.
Following the medical history, a physical should be performed, specifically inspection and palpation. Inspecting the pelvic area while the patient undergoes attempted contraction and relaxation of the pelvic muscles can reveal asymmetries, prolapse, or inability to control the actions of the muscles. Palpation of these muscles may elicit involuntary contraction (spasms), identify areas of weakness, or elicit pain. The aforementioned symptoms/signs are positive findings for PFD.
"
When the muscles of the pelvic floor no longer function properly, it can lead to urinary incontinence, fecal incontinence, sexual dysfunction, and pelvic organ prolapse.
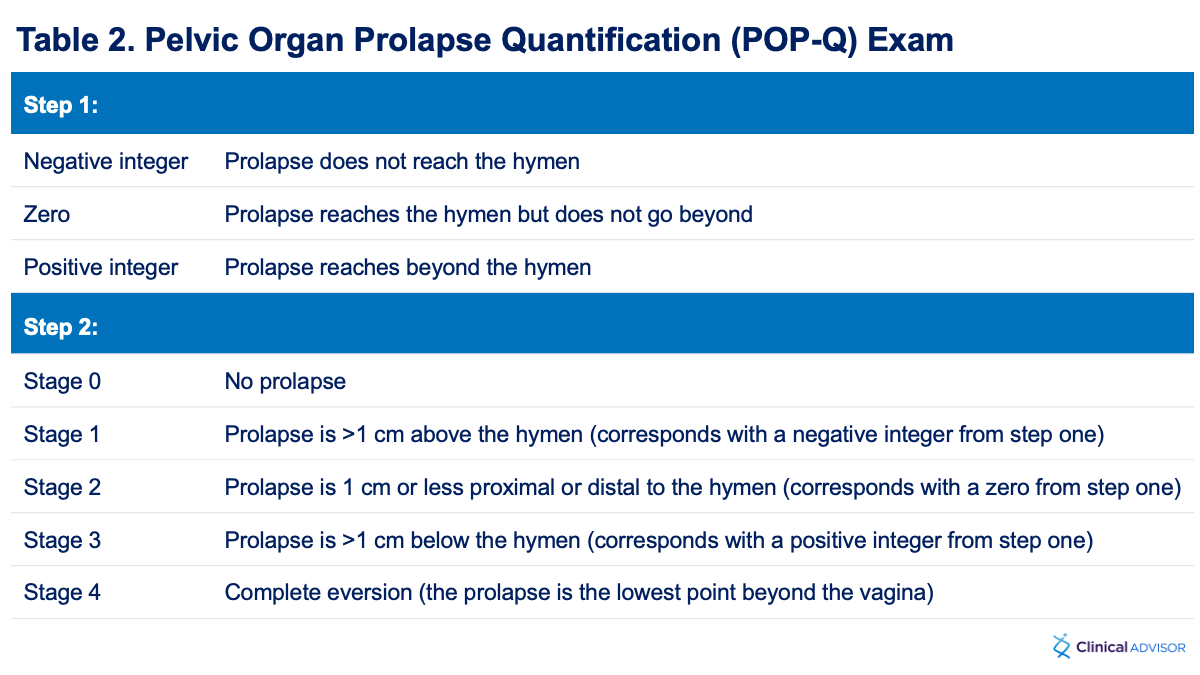
If the primary symptom is prolapse, the pelvic organ prolapse quantification exam (POP-Q) should be referenced to determine the stage and severity of the prolapse (Table 2). The POP-Q exam is divided into 2 parts. During the first part of this exam, the prolapse is measured during Valsalva maneuver and then assigned an integer based on how far the prolapse reaches in relation to the hymen. The second part of the exam includes staging the prolapse based on established criteria. Utilization of the POP-Q exam can help guide treatment.10
Treatment Options
There are multiple options available for the treatment of PFD. Choosing an option should be individualized to address the patient’s primary symptom. It is crucial to customize treatment to maximize the patient’s ability to adhere to treatment, as some treatments may be uncomfortable or costly. Each option should be discussed between the provider and the patient to ensure appropriate care.
Pelvic Floor Physical Therapy
Pelvic floor physical therapy (PT) is the first-line recommendation for treatment and prevention of PFD, either as monotherapy or as adjunctive therapy.11 Physical therapy is highly effective when completed with proper technique and follow-up. The PT regimen should be guided by the patient’s presenting symptoms and aim to improve control of the pelvic floor muscles to ameliorate the symptoms of PFD.12
Weight Loss
Because obesity can play a role in the etiology of PFD, decreasing BMI reduces the risk for developing PFD and the severity of symptoms. Both surgical and nonsurgical weight loss options have been shown to improve the symptoms of PFD.13 Nonsurgical options include diet changes and exercise regimens, both of which should be discussed with the patient.
Pessary
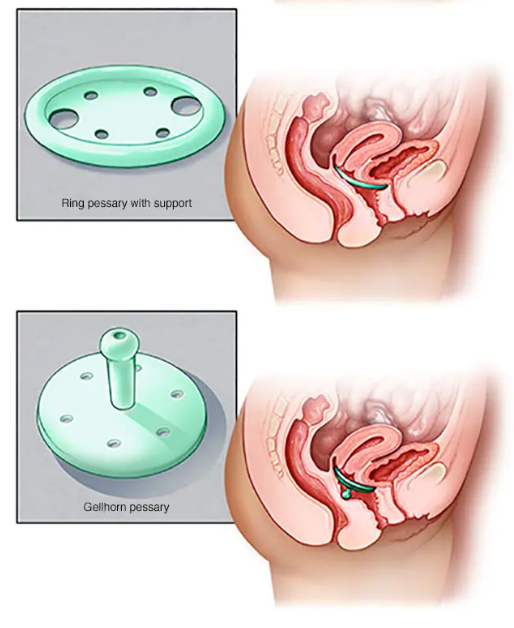
The pessary is inserted into the vagina and provides support to the prolapsed area(s).13 Pessaries come in variable shapes, but the ring pessary and the Gellhorn pessary (Figure 2) are the most widely used for PFD.14 Both types of pessaries decrease symptoms of urinary incontinence and improve prolapse.15 Pessaries require a fitting and require ongoing care to avoid vaginal irritation and infection. With proper education and follow-up, pessaries are suitable treatment options for some forms of PFD.
Figure 2. Illustrations of the ring and Gellhorn pessaries for pelvic organ prolapse. Source: Used with permission of Mayo Foundation for Medical Education and Research. All rights reserved.14
Surgery
Surgery is an option for women with pelvic organ prolapse who are refractory to other treatments, or for those who desire a more immediate response to treatment. There are a multitude of surgical options for these patients and choosing the best option will depend on the type and severity of the prolapse. Some options include sacral colpopexy, uterosacral or sacrospinous ligament suspension, anterior vaginal prolapse repair, posterior vaginal prolapse repair, and colpocleisis.15 Pelvic organ prolapse suspension can greatly improve sexual function in patients with PFD and can improve incontinence.16 One study found that 81% of women with severe prolapse who opted for surgical correction saw significant improvement in their symptoms, and these findings were consistent regardless of the procedure used.17 Surgical options are more invasive and should be discussed on an individual basis to determine what is right for the patient.
Conclusion
The musculature of the pelvic floor is vital for everyday functions. When these muscles no longer work properly, urinary incontinence, fecal incontinence, pelvic organ prolapse, and sexual dysfunction can occur. The result can decrease quality of life by affecting physical, psychological, social, and financial wellbeing. It is important for health care providers to promptly diagnose PFD and tailor treatment to limit the burden the disorder can place on patients.
"
["post_title"]=>
string(65) "Female Pelvic Floor Dysfunction and its Effect on Quality of Life"
["post_excerpt"]=>
string(147) "The pelvic floor musculature plays a crucial role in many activities of daily living and can cause tremendous distress in the event of dysfunction."
["post_status"]=>
string(7) "publish"
["comment_status"]=>
string(6) "closed"
["ping_status"]=>
string(6) "closed"
["post_password"]=>
string(0) ""
["post_name"]=>
string(40) "pelvic-floor-dysfunction-quality-of-life"
["to_ping"]=>
string(0) ""
["pinged"]=>
string(0) ""
["post_modified"]=>
string(19) "2024-04-05 12:31:59"
["post_modified_gmt"]=>
string(19) "2024-04-05 16:31:59"
["post_content_filtered"]=>
string(0) ""
["post_parent"]=>
int(0)
["guid"]=>
string(45) "https://www.clinicalpainadvisor.com/?p=117280"
["menu_order"]=>
int(0)
["post_type"]=>
string(4) "post"
["post_mime_type"]=>
string(0) ""
["comment_count"]=>
string(1) "0"
["filter"]=>
string(3) "raw"
}
[2]=>
object(WP_Post)#7835 (24) {
["ID"]=>
int(117112)
["post_author"]=>
string(5) "45524"
["post_date"]=>
string(19) "2024-03-29 11:20:00"
["post_date_gmt"]=>
string(19) "2024-03-29 15:20:00"
["post_content"]=>
string(12271) "
As the global population becomes older, physicians are increasingly navigating the complexities of geriatric medicine. Older adults often have multiple chronic conditions that require ongoing treatment, which frequently results in the practice of polypharmacy — typically defined as the concurrent use of 5 or more medications.1
Although polypharmacy begins as a well-intentioned effort to manage cooccurring conditions, the interaction of these different medications can become a health hazard instead of an optimal solution. Given the increased risks for adverse drug interactions, medication errors, and cognitive impairment, addressing polypharmacy and developing a nuanced approach to geriatric care is crucial to safeguarding the health of older adults.
Increasing Prevalence of Polypharmacy in Older Adults
In a chapter on polypharmacy published in Geriatric Rehabilitation, co-authors Parulekar and Rogers noted that while only 13% of the United States population was aged 65 years and older, this age group accounted for 33% of total prescription medications.2 More than 50% of older adults with multimorbid conditions receive 5 or more medications, with the rate varying between 10% and 55% globally.3 Furthermore, a study of survey data from the Centers for Disease Control and Prevention (CDC) found that the majority of older adults in the US had major polypharmacy and nonsteroidal anti-inflammatory drugs (NSAIDs) were the most common medication type.4
The prevalence of polypharmacy is even higher among women. Research suggests that women are more likely than men to require more than 1 or more specialized medications,1 and older women have higher rates of multimorbidity relative to men — with a consequently higher prevalence of polypharmacy.5
"
Managing polypharmacy requires careful monitoring and coordination by health care providers to deprescribe, optimize medication regimens, and minimize risks for patients.
Erika Ramsdale, MD, an associate professor at the Department of Medicine, Hematology/Oncology at the University of Rochester Medicine, has studied the effects of polypharmacy on older adults initiating cancer treatment6 and spoke about this issue. “Polypharmacy and potentially inappropriate medications are very, very common in older adults, and especially within certain populations, such as older adults with cancer. [However], there is not an easy way to estimate the burden of medication-related adverse effects on patients and the health care system as a whole,” she remarked.
Identifying Polypharmacy Risks and Related Comorbidities
Risk factors for polypharmacy include both patient-level factors (eg, increased age, difficulty self-managing medications, multimorbidity, disabilities) as well as health care system-level components, such as poor continuity of care, prescribing cascades, the use of multiple pharmacies, and inadequately updated medical records.7,8
While polypharmacy is often deemed necessary to treat multimorbidity, the concurrent use of medications has been shown to cause harm in and of itself. In a retrospective cohort study published in 2023, older adults who received multiple medications experienced significantly higher rates of severe comorbidity relative to those who did not experience polypharmacy. Patients with polypharmacy also had a greater rate of all-cause hospitalizations and emergency department (ED) visits.9
Polypharmacy also carries specific neurologic and psychiatric risks. Older adults with polypharmacy and multimorbidity demonstrate greater levels of cognitive impairment, relative to their peers with fewer comorbidities and medications,10 and has been associated with worse self-reported health and depression in older adults.11
Given the risks associated with multiple medications in older adults, many experts have called into question the “appropriate” vs “inappropriate” use of polypharmacy.2 To this aim, Mohamed and colleagues conducted a study to examine the associations between polypharmacy, potentially inappropriate medications, and adverse treatment outcomes in a large national cohort of older adults with advanced cancer. They found that 67% of patients received 1 or more inappropriate medications, and the use of inappropriate medications increased the odds of unplanned treatment-related hospitalization. Additionally, polypharmacy overall was associated with increased risk for postoperative complications, hospitalizations, and mortality risk.8
Dr Ramsdale emphasized the importance of not just the number of medications prescribed to a patient, but also their appropriateness. “Some patients have polypharmacy by number, but all their medications are needed and appropriate.”
Further complicating this medication management issue, Dr Ramsdale addressed the challenge of differentiating between patients who develop symptoms from polypharmacy vs a root cause issue, such as comorbidities/disease. “Often, there is not one ‘root cause’ for a symptom or adverse effect in older adults. There are generally multiple contributing factors and you have to look at all of them and also how the factors interact with each other. One thing you can say is that medications are very often contributing and need to be considered each time something happens.”
Concerns & Barriers in the Management of Polypharmacy in Clinical Practice
Although a wealth of evidence has demonstrated the adverse health risks associated with polypharmacy, the question remains as to how health care systems should best manage this issue. Researchers conducted a study across 14 countries, including the US and UK, to identify the barriers associated with addressing polypharmacy in primary care. They found the most common barriers were a lack of evidence-based guidance, a lack of communication and decision-making systems, and gaps in support.12
From a clinician’s perspective, Dr Ramsdale stated,
Older adults tend to have many doctors who are all prescribing [medications], sometimes in different health systems, leading to fragmentation of care. Providers also may not want to alter [a medication] that another provider has prescribed.
In-depth review of medications takes a lot of time and thought, as each patient’s situation is unique and everyone has different goals and preferences. In addition, clinicians often do not have the time or resources to accomplish this for all patients because of the way our health care system is set up and [the type] of care it prioritizes.
Because one of the major concerns regarding polypharmacy is the increased risk for drug-to-drug interactions that are associated with adverse events and even death,13 there is a critical need to support physicians in these complicated — but increasingly common — cases of medication management.
How Can Providers Manage Polypharmacy in Older Adults?
Researchers have agreed that screening and interventional tools to optimize medication usage for improved outcomes may be beneficial.9 However, the frequency of prescribing multiple medications needs to be evaluated to reduce adverse events and medication burden in this patient population.4 Clinical studies have shown that one of the ways of reducing exposure to polypharmacy is through the practice of “deprescribing” medications.12
Deprescribing medications involves the identification of inappropriate or unnecessary medications to ultimately taper or discontinue their use. In 2019, the American Academy of Family Physicians (AAFP) developed recommendations for clinicians to help in deprescribing medications and reducing the risks for polypharmacy.7 Some of the key guidelines include the identification and prioritization of medications to discontinue, conducting informed decision-making with the patient, ensuring routine follow-up visits, and considering the risks vs benefits when refilling medications.
One of the key aspects in reducing polypharmacy is medication reconciliation, which can be more effectively achieved by improving the communication between provider and patient and the process of discharge from hospitalization. With the increased use of artificial intelligence and clinical decision support systems, the risks for polypharmacy may be minimized.14
Given that many older patients experience some degree of polypharmacy, pharmacists, specialist nurses, and physician assistants play a vital role in medication management, quality prescribing practices, and safety monitoring.4 Managing polypharmacy requires careful monitoring and coordination by health care providers to deprescribe, optimize medication regimens, and minimize risks for patients. Overall, polypharmacy in older adults is directly related to health care service outcomes,9 which warrants the need for a multidisciplinary, holistic approach to address and evaluate its use among patients.
What’s the best way to curb vaping, especially among adolescents and young adults?
Despite Food and Drug Administration (FDA) regulation, vaping is flourishing, with a steady stream of e-cigarette products finding their way into stores as well as into the hands, lungs, and bloodstreams of America’s youth. Vaping, it seems, is the new smoking for teenagers and young adults.
“E-cigarettes have taken over the youth tobacco use landscape. They are the most commonly used tobacco product,” said Thomas Carr, Director of National Policy at the American Lung Association (ALA), in an exclusive interview.
Although there is not yet data to show whether vaping is as harmful as cigarette smoking, substantial harms have been documented — enough to show that vaping poses a threat to human health, especially to the lungs and the heart.1
Given that February has been designated by the Centers for Disease Control and Prevention (CDC) as heart health month, this report looks at what is being done — and what could be done — to curb youth vaping.
"
Taxation has worked well at reducing use in every other tobacco product, especially among youth. I feel pretty confident in saying it will reduce vaping rates.
“The [American Lung] Association is committed to reducing and eliminating use of e-cigarettes among youth users,” noted Carr. Moving forward, he added, the ALA is hoping to see:
better FDA regulation and enforcement with respect to e-cigarettes;
high levels of taxation on e-cigarettes;
an end to the sale of flavored e-cigarettes (a measure that has been taken by only 5 states thus far);
incorporating vaping into existing state tobacco-control programs;
more media campaigns against e-cigarette use; and
community education in schools about the dangers of vaping.
The American Heart Association (AHA) is similarly dedicated to curbing youth vaping, said Rose Marie Robertson, MD, AHA Science and Medical Officer, in an exclusive interview. “A comprehensive approach is needed to help reduce vaping among young people,” she said.
“We have heard from young people who recognize the dangers of vaping and their own addiction to these products, but don’t feel like they know the proper strategies to quit or even how to say no to e-cigarettes and other dangerous products to begin with,” said Robertson. “Therefore, our efforts focus on significant investments in research, youth engagement efforts, and support for schools to choose restorative rather than punitive approaches to students who vape,” she noted.
The AHA and the ALA are also united in their desire for better regulation and enforcement of vaping by the FDA and states.
Statistics on Youth Vaping
Although there has been “some decline since 2019” in the use of e-cigarettes, said Carr, “e-cigarettes remain the most commonly used tobacco product.”
CDC’s 2023 National Youth Tobacco Survey confirms that e-cigarettes are the most commonly used tobacco product by youth in the US. The 2023 survey found that 10% of high school students and 4.6% of middle school students used e-cigarettes. Notably:2
25.2% of current youth e-cigarette users used an e-cigarette product every day;
34.7% of youth e-cigarette users surveyed reported using e-cigarettes during at least 20 of the previous 30 days;
89.4% of youth users used flavored e-cigarettes; fruit flavors were most popular, followed by candy, desserts/other sweets, mint, and menthol;
57.9% reported using products with “ice” or “iced” in the branding;
the most common e-cigarette devices used were disposables (60.7%) followed by prefilled/refillable pods (16.1%); and
the most popular brands included Elf Bar (56.7%), Esco Bars (21.6%), Vuse (20.7%), JUUL (16.5%), and Mr. Fog (13.6%).
Taxation
One under-utilized strategy that may effectively curb the use of e-cigarettes by both youths and adults is heavy taxation — meaning taxation at the same level as cigarettes, said Carr.
Currently, there is no federal tax on e-cigarettes, and only 31 states and the District of Columbia have enacted excise taxes on vaping products.3 The level of taxation varies widely, with some surcharges hardly noticeable, said Carr.
According to the Tax Foundation, a nonprofit organization that researches tax policy in the US and elsewhere, methods used to tax vaping vary. “Authorities tax based on manufacturer, wholesale, or retail price (ad valorem), volume (specific), or with a bifurcated system that has different rates for open and closed tank systems,” noted a Tax Foundation blog on vaping taxes. “Of those that tax wholesale values, Minnesota levies the heaviest tax at 95 percent, followed closely by Vermont at 92 percent. On the other end of the spectrum, Connecticut levies a 10 percent wholesale tax and Wyoming applies a 15 percent wholesale tax.”
Other states levy a per mL tax. The states with the lowest per milliliter (mL) taxations are Delaware, Kansas, North Carolina, and Wisconsin, with a rate of $0.05 per mL. Louisiana has the highest rate per mL, after tripling this rate to $0.15 per mL in 2023, the blog noted.3
“Taxation has worked well at reducing use in every other tobacco product, especially among youth. I feel pretty confident in saying it will reduce vaping rates,” said Carr. “We’re still sorting through what completely works,” he added.
FDA regulation
The FDA is acutely aware of the dangers that e-cigarettes pose to youth. A focused segment of their Comprehensive Plan for Tobacco and Nicotine Regulation aims to prevent youth from accessing e-cigarettes and other tobacco products. The FDA has claimed that “significant regulatory and research efforts related to access, marketing, and education are already underway.”4
Regulation enforcement for e-cigarettes is a stated FDA priority. As former FDA Commissioner Scott Gottlieb, MD, said in a 2019 press release, “As the number of children using e-cigarettes remains at epidemic levels, our enforcement work has been one cornerstone of our efforts to protect youth from the dangers of tobacco products.” Gottlieb noted that the FDA had been involved in “vigorous enforcement efforts.” These included “a number of actions to combat the illegal sales of e-cigarettes to youth at brick-and-mortar and internet storefronts, as well as steps to target companies engaged in kid-friendly marketing that can increase the appeal of these products to youth,” and other actions “focused on both retailers and manufacturers.”5
In its Guidance for Industry issued in April 2020, the FDA laid out its enforcement priorities, announcing its intent to target any electronic nicotine delivery system (ENDS) product being sold after September 9, 2020, “for which the manufacturer has not submitted a premarket application.”6
FDA’s Guidance for Industry also stated that for products marketed “without FDA authorization, FDA intends to prioritize enforcement against: [1] Any flavored, cartridge-based ENDS product (other than a tobacco- or menthol-flavored ENDS product); [2] All other ENDS products for which the manufacturer has failed to take (or is failing to take) adequate measures to prevent minors’ access; and [3] Any ENDS product that is targeted to minors or whose marketing is likely to promote use of ENDS by minors.”6
ALA, AHA: More Regulation, Better Enforcement Needed
Although the ALA is pleased that the FDA has not approved any flavored tobacco products to date, the FDA hasn’t yet enforced against any of these products, said Carr, who noted that the ALA would like to see a ban on the sale of all flavored tobacco products.7
“The Lung Association has been dismayed at the delay with the FDA, although they have been making more progress recently. In some cases, the companies aren’t following the laws at all and selling products without premarket review. A lot of these products come from overseas so they’re hard to interdict — especially flavored disposable varieties,” said Carr.
Dr Robertson of the AHA echoed this sentiment. “While the FDA has fined retailers for continuing to sell unauthorized tobacco products, the agency must be given the proper resources to not only fund additional research on characterizing flavors, but also strengthen enforcement efforts to remove all illegal e-cigarettes from the marketplace,” she said.
“The [AHA] has continued to urge the Food and Drug Administration to complete its review of all e-cigarette product applications and we are working to ensure that state laws align with the federal minimum age for sale of tobacco products, which is 21,” she added.
E-Cigarette Smuggling
The smuggling of e-cigarettes across the border into the US complicates vaping regulation enforcement.7
“The Lung Association was pleased by the FDA announcement in May 2023 that e-cigarette products from several companies — Elf Bar, Esco Bar and Eon Smoke — were added to an FDA import alert red list with CBP [Customs and Border Protection] in order to be detained at the border without conducting a full inspection at the time of entry. Additional e-cigarette products have been added to the list,” stated the ALA’s State of Tobacco Control 2024 Report.7
“However, Elf Bar, the most popular e-cigarette with kids in 2023, was able to avoid enforcement initially by simply changing the name of its product, a disturbing loophole that needs to be closed. A recent US Department of Health and Human Services Inspector General report looked at FDA enforcement against retailers from 2010 to 2020, and found that FDA did not always follow through with more serious penalties such as civil monetary,” the ALA report continued.7
To date, the FDA and Customs and Border Protection have worked together to seize 1.4 million illegal cigarette products at the border, the report noted.7
The Manufacturers Strike Back
Taking a page from the litigation playbook of big tobacco companies, many e-cigarette manufacturers have filed lawsuits against FDA marketing denial orders for flavored e-cigarettes. The ALA has signed more than 20 amicus briefs with coalition partners in 2022 and 2023 asking courts to uphold these orders. To date, 6 of 8 US circuit courts have upheld these FDA marketing denial orders.7
In addition to leveraging litigation to fight to keep flavored e-cigarettes on retail shelves, manufacturers have kept on top of youth trends and interests when marketing their products to ensure sales. “They have proven expert at getting around regulations whenever they can by innovating their products,” Carr lamented.
Dr Robertson of the AHA agreed. “Big Tobacco and the vaping industry continue to foster addiction in younger generations by developing and marketing new tobacco products that appeal to youth and get them addicted.” This, of course, is nothing new, she added. “For decades, the tobacco industry has modified old products and created new ones to hook new users and keep them addicted, leading to tobacco use as a leading cause of preventable disease and death and a major risk factor in the development of heart disease and stroke.”
Second-Hand Vape
An issue of note that has yet to be talked about is the dangers of second-hand vape, said Carr. “Second-hand aerosol isn’t harmless,” he noted. This problem can be addressed by “adding e-cigarettes to smoke-free workplace laws that exist in a number of states … to prevent vaping in restaurants and other public places.”7
Public and Patient Outreach
Public outreach and education are imperative in the battle against rising rates of e-cigarette use in youth, said Carr. This includes efforts by clinicians, community education in schools, peer education on the dangers of tobacco and smoking, and the use of media campaigns.
One such media campaign is #DoTheVapeTalk.8 The American Lung Association (ALA) recently paired with the nonprofit Ad Council to launch this youth vaping awareness campaign, which involves a public service announcement showing how a dad talks to his teen about the dangers of vaping. #DoTheVapeTalk arms parents with the necessary facts to discuss the dangers of vaping with their kids “while they’re still willing to listen,” according to the ALA State of Tobacco Control 2024 report.7 Unfortunately, there is a paucity of youth-cessation resources like #DoTheVapeTalk, Carr noted.
“It’s vital that the harms and consequences of e-cigarettes and other addictive tobacco products be shared by trusted messengers, such as doctors and other health professionals, teachers, coaches and parents,” said the AHA’s Robertson. “But it is just as important that these influencers in young people’s lives specifically encourage them to quit and refer them to the proper resources and care to do so.”
Carr urged clinicians to take an active role in public and patient outreach. In particular:
When seeing kids in the office, physicians should ask about tobacco use and vaping, assess their desire to quit, and refer to counseling.
Pediatric pulmonologists can share stories about patients and vaping in the form of letters to the editor or community outreach.
Clinicians can support public policy efforts.
"
["post_title"]=>
string(80) "Protecting Youth From the Dangers of Vaping: What’s Been Done, What’s Needed"
["post_excerpt"]=>
string(171) "In recognition of the CDC’s designation of February as American Heart Month, this report looks at what is being done — and what could be done — to curb youth vaping."
["post_status"]=>
string(7) "publish"
["comment_status"]=>
string(6) "closed"
["ping_status"]=>
string(6) "closed"
["post_password"]=>
string(0) ""
["post_name"]=>
string(28) "protecting-youth-from-vaping"
["to_ping"]=>
string(0) ""
["pinged"]=>
string(0) ""
["post_modified"]=>
string(19) "2024-03-22 11:45:35"
["post_modified_gmt"]=>
string(19) "2024-03-22 15:45:35"
["post_content_filtered"]=>
string(0) ""
["post_parent"]=>
int(0)
["guid"]=>
string(45) "https://www.clinicalpainadvisor.com/?p=116973"
["menu_order"]=>
int(0)
["post_type"]=>
string(4) "post"
["post_mime_type"]=>
string(0) ""
["comment_count"]=>
string(1) "0"
["filter"]=>
string(3) "raw"
}
}
Enjoying our content?
Thanks for visiting Clinical Pain Advisor. We hope you’re enjoying the latest clinical news, full-length features, case studies, and more.
You’ve viewed {{metering-count}} of {{metering-total}} articles this month. If you wish to read unlimited content, please log in or register below. Registration is free.
{{login-button}} {{register-button}}
Log in to continue reading this article.
Don’t miss out on today’s top content on Clinical Pain Advisor. Register for free and gain unlimited access to:
- Clinical News, with personalized daily picks for you
- Case Studies
- Conference Coverage
- Full-Length Features
- Drug Monographs
- And More
{{login-button}} {{register-button}}
Want to read more?
Please login or register first to view this content.